

International Journal of Scientific Pediatrics
COMBINED GENETIC DISORDERS IN PATIENTS WITH COAGULOPATHYЕЙ
Makhmudova A.D.
1
, Berger I.V.
2
, Madasheva O.G.
3
, Ulugova Sh.T.
4
1. Doctor of Medical Sciences, Deputy Director for the Scientific Department of the
RSNPMC of Hematology.
2. Doctor of Philosophy (PhD) of Medical Sciences, Deputy Chief Physician at the
Republican Scientific and Practical Medical Center for Hematology (RNPMCH) of the
Ministry of Health of the Republic of Uzbekistan.
3. Doctoral student at the Republican Scientific and Practical Medical Center for
Hematology (RNPMCH) of the Ministry of Health of the Republic of Uzbekistan.
4. Doctor of the higher category. doctoral student at the Republican Scientific and Practical
Medical Center for Hematology (RNPMCH) of the Ministry of Health of the Republic of
Uzbekistan,
Academic Editor:
Arzikulov A.
Professor, Andijan State Medical
Institute
Received:
20 may 2022
Accepted:
27 May 2022
Published:
31 May 2022
Publisher’s Note:
IJSP stays
neutral with regard to jurisdictional
claims in published maps and
institutional affiliations.
Copyright:
© 2022 by the
authors. Licensee IJSP, Andijan,
Uzbekistan. This article is an open
access article distributed under
the terms and conditions of the
Creative Commons Attribution
(CC BY) license (https://creative-
commons.org/licenses/by/4.0/).
Abstract.
The article presents the available literature data on combined pathologies with
hereditary coagulopathy and includes our own statistical calculations and 4 clinical cases
of a combination of Hemophilia A, von Willebrand disease with hard palate defects, the
genetic locus of which is located in the immediate vicinity of the F8 gene. Mutations
and changes in the protein structure of the F8 gene can lead to the development of
both sporadic forms of hemophilia and occur in patients with a hereditary predisposition.
Research methods: coagulological, examination and questionnaire data. Conclusion: it
is necessary to widely introduce methods of molecular genetic research and prenatal
diagnostics in Uzbekistan.
Key words:
F8 gene, Hemophilia A, von Willebrand disease, hereditary pathologies,
chromosomal disorders, cleft palate, color blindness.
Article
OPEN ACCESS
published: 31 May 2022
doi.org/10.56121/2181-2926-2022-1-23-29
May 2022 / Issue 01 / Article 03
23
IJSP
Introduction.
The X chromosome contains 867 identified genes;
most of these genes are responsible for the development of tissues
such as bones, nerves, blood, liver, kidneys, retina, ears, ear, heart,
skin, and teeth. There are at least 533 disorders due to the involvement
of genes on the X chromosome. A «trait» or «disorder» defined by a
gene on the X chromosome demonstrates X-linked inheritance [1].
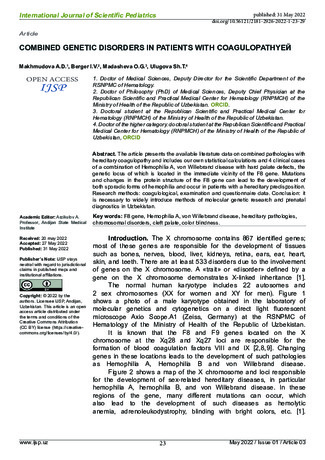
The normal human karyotype includes 22 autosomes and
2 sex chromosomes (XX for women and XY for men). Figure 1
shows a photo of a male karyotype obtained in the laboratory of
molecular genetics and cytogenetics on a direct light fluorescent
microscope Axio Scope.A1 (Zeiss, Germany) at the RSNPMC of
Hematology of the Ministry of Health of the Republic of Uzbekistan.
It is known that the F8 and F9 genes located on the X
chromosome at the Xq28 and Xq27 loci are responsible for the
formation of blood coagulation factors VIII and IX [2,8,9]. Changing
genes in these locations leads to the development of such pathologies
as Hemophilia A, Hemophilia B and von Willebrand disease.
Figure 2 shows a map of the X chromosome and loci responsible
for the development of sex-related hereditary diseases, in particular
hemophilia A, hemophilia B, and von Willebrand disease. In these
regions of the gene, many different mutations can occur, which
also lead to the development of such diseases as hemolytic
anemia, adrenoleukodystrophy, blinding with bright colors, etc. [1].

Rice. 1 Chromosome set of a healthy person, male karyotype, normal (46, XY).
The photo was taken in the Laboratory of Molecular Cytogenetics of the Republican
Scientific and Practical Center for Hematology of the Ministry of Health of the Republic
of Uzbekistan. Ph.D. Assesorova Yu.Yu.
Rice. 2 X-chromosome with an ideogram. Location of the F8 and F genes 9. The arrows
mark the Xq28 and Xq2 loci responsible for the development of hemophilia A and B.
P is the short arm, q is the long arm. Dark and light stripes are segments conditionally
taken as a gene. Photo taken by Ph.D. Assesorova Yu.Yu. in the laboratory of molecular
cytogenetics of the SRCPM of Hematology of the Ministry of Health of the Republic of
Uzbekistan.
27 exons contains the F8 gene and encodes two alternative transcripts.
The first option contains instructions for making the large glycoprotein
isoform A, the ß-globulin (antihemophilic globulin) protein, which is called
coagulation factor VIII. The second transcript encodes a small protein
(isoform B), which mainly consists of the phospholipid-binding domain of
factor VIIIa and is required for coagulant activity [1,8].
The F8 gene can be called by its content as a “gene within a gene”,
since an RNA gene (MIR1184-1) and two pseudogenes (EEF1A1P31,
LOC100419792) are nested in its structure, and 2 protein-coding genes
(F8A1) are located on the opposite positive strand , H2AB1) and 2
recombination regions (LOC106146150, LOC106146143). Coagulation
factor VIII is composed of multiple Cu-oxidase (CuRO) and FA58C
domains. This protein circulates in the blood in an inactive form, which is
associated with another molecule, von Willebrand factor [7].
Changes in these genes of factors VIII and IX, leading to the
International Journal of Scientific Pediatrics
May 2022 / Issue 01 / Article 03
24
published: 31 May 2022

International Journal of Scientific Pediatrics
May 2022 / Issue 01 / Article 03
25
published: 31 May 2022
development of pathology, can be represented by single nucleotide
substitutions that change the reading frames, deletions of chromosome
fragments containing these loci, inversions, and other genetic
rearrangements [12]. Until recently, the genetic diagnosis of hemophilia,
taking into account the subtype of the disease, was difficult due to the
fact that the construction of this gene is extremely complex and rather
voluminous, and also due to the wide range of potential mutations. An
effective study of the genetic determinant of the disease has become
possible due to the development of DNA sequencing techniques and the
improvement of molecular cytogenetic equipment.
M.J. McGinniss et all. (USA, 1993) it was shown that 40% of patients
with severe hemophilia A, who previously failed to identify any mutation
during screening or sequencing, have inversions of the F8 gene. Patients
have one of two major inversions—with a breakpoint in intron 22 or with
a breakpoint in either of the two copies of the F8 gene (Inversion with a
breakpoint in the distal portion of the F8 gene is the more common variant)
[7]. These inversions explain why deletions and point mutations have not
yet been found in such patients and why transcription of intron 22 and
exon 23 is impossible [11].
Quite a few cases of a combination of congenital FVIII deficiency and
color blindness are known in the world [12], since the segments responsible
for color perception and hemophilia gene loci are quite close to each other.
The OPN1LW, OPN1MW, and OPN1SW genes code for red, green, and
blue-sensitive receptors. Mutations in the OPN1LW and OPN1MW genes
lead to the development of red-green color blindness, and in the OPN1SW
gene, blue-yellow color blindness. If a mutation simultaneously affects two
genes, OPN1LW and OPN1MW, monochromasia develops [2].
Back in 1991, when working with data from the decoding of the human
genome, a gene was found that is also located on the X chromosome and
is responsible for the development of the “cleft palate” - an altered TBX22
gene [1].
Cleft palate is one of the most common congenital malformations
and, according to different authors, occurs in 1 born baby per 1000, which
is 0.1%, most of which are boys [6]. In some European regions (Denmark,
Czech Republic) and the Russian Federation, these figures are an order
of magnitude higher, and 1 child out of 600–700 babies is born with this
defect, and half of them also have a defect in the form of a cleft lip [3].
Most often, the cleft palate is registered in infants born in Asia and North
America, and is almost never found among the inhabitants of Africa [4].
The results of whole genome sequencing conducted in 2004 in
Scandinavia from 574 families from 13 populations showed the relationship
of different loci of chromosomes 1, 2, 4, 6, 14, 17 and 19 (IRF6, TGF-α,
MSX1, T-βr1, FOXFE1, RTCH, ROR2, TGF-β3, RARA, PVRL1) with the
risk of developing non-syndromic congenital cleft lip with/without palate
[5]. Some of the candidate genes in the development of facial cleft belong
to the growth factor genes (TGF-α, TGF-β3) and transcription factor genes
(MSX1, IRF6, TBX22), some to the genes that control the synthesis of
enzymes involved in the metabolism of xenobiotics (CYP1A1, GSTM1,
NAT2) or folic acid (MTHFR), some of the genes regulate the div’s immune
responses (PVRL1, IRF6) [10]. Studies of IRF6 gene polymorphisms have
also revealed associations with congenital cleft palate in many populations

International Journal of Scientific Pediatrics
May 2022 / Issue 01 / Article 03
26
published: 31 May 2022
[5].
Own data.
In 2010, our research group created and is still maintaining
an electronic national register of patients with hemophilia and other
coagulopathies covering all regions of the Republic of Uzbekistan.
Research methods:
coagulological, examination and questionnaire
data.
According to our registry, by the end of 2021, 1987 patients with
hereditary coagulopathy are registered. Analysis of the data showed that
among all patients - 30% are sporadic cases of the onset of diseases.
Since hemophilia is not always registered at the birth of a child, moderate
and mild forms of the disease can be detected at the age of 3, we provide
statistical data for 2019. According to the State Statistics Committee,
815.9 thousand newborns were born in the Republic of Uzbekistan in
2019. The number of registered patients born in 2019 was 16 patients
with Hemophilia A, 5 patients with Hemophilia B and 29 children with von
Willebrand disease. Thus, there are 6 children suffering from hemophilia
per 100,000 newborns in Uzbekistan, while according to world statistics,
this figure is 10:100,000 newborns. 50% of all cases reported each year
are severe (i.e. less than 1% of clotting factors).
Among the patients of the Republic, children with Hemophilia A and
von Willebrand disease with combined pathology in the form of a cleft
palate (cleft palate) were identified. 2 patients diagnosed with hemophilia
A and 2 patients with von Willebrand disease. Patients with hereditary
coagulopathy and color blindness were not registered in the Republic of
Uzbekistan.
Child, 11 months (2020). von Willebrand disease, factor VIIIa level of 3%, and complete
cleft palate. Heredity is favored through the maternal line. Also in the family there are 2
more children with a mild severity of the disease, without pathology of the hard palate.

International Journal of Scientific Pediatrics
May 2022 / Issue 01 / Article 03
27
published: 31 May 2022
Child, 2021 Hemophilia A severe (factor VIII level - 1%), heredity is not traced.
Complete cleft palate.
Child, 4 years old (2018). von Willebrand disease, factor VIIIa 7%, and partial cleft
palate. Heredity is burdened, there are cases of the disease in male relatives on the
maternal side.
Child, born in 2016 Hemophilia A factor VIII level - 3%, and complete cleft palate.

International Journal of Scientific Pediatrics
May 2022 / Issue 01 / Article 03
28
published: 31 May 2022
Heredity is burdened. The child underwent a successful operation and restoration of
the defect. The operation was carried out under constant monitoring of hemostasis
parameters and the corresponding administration of blood coagulation factor
preparations.
The only treatment for such patients with congenital pathology of the
palate is surgery with suturing the defect or installing an implant. For patients
with a deficiency of blood coagulation factors, these operations should be
carried out exclusively with the replacement of an adequate amount of
blood coagulation drugs, at the rate of 50-60 mg / kg - at least 3 times a
day. It is recommended to maintain the missing clotting factor at least 50%
for a minimum of 14 days. Otherwise, the operation may be complicated
by profuse bleeding, failure of the sutures and the development of other
complications associated with the failure of the coagulation link of hemostasis.
With timely surgical intervention and defect plasty, this anomaly does
not pose a danger to life. If the defect is not corrected in time, then numerous
complications and inflammatory diseases of the nasopharynx develop.
Conclusion:
The solution to this problem is the possibility of
determining X-linked diseases before the birth of a child. For all regions of
Uzbekistan and neighboring countries of the CIS, it is necessary to introduce
mandatory molecular genetic testing for chromosomal pathologies for
all couples entering into marriage and persons with a predisposition to
hereditary diseases, as well as to actively introduce prenatal diagnostics.
Prenatal diagnosis will allow, long before the moment of birth, to find
out whether everything is in order with the health of the child or whether
he has inherited any pathological abnormalities in the genetic material.
Bibliography:
1. Гороховский А.Н. Ген F8: [Электронный ресурс] // ГЕНОКАРТА
Генетическая энциклопедия. 2020. – URL: https://www.genokarta.ru/
gene/F8.
2. Масленников Д.Н. Дальтонизм: [Электронный ресурс] //
ГЕНОКАРТА Генетическая энциклопедия. 2022. – URL: https://www.
genokarta.ru/disease/Daltonizm.
3. Таалайбеков, Н. Т. Статистика рождаемости детей с
врожденными пороками развития и использование современных
технологий в реабилитации / Н. Т. Таалайбеков, А. М. Ешиев. — Текст
: непосредственный // Молодой ученый. — 2016. — № 3 (107). — С.
310-312. — URL: https://moluch.ru/archive/107/25592
4. Chapel Hill// American Cleft Palate-Craniofacial Association.
Parameters for evaluation and treatment of patients with cleft lip/palate
or other craniofacial anomalies. Revised edition, Nov 2009., NC. P.
1-34. https://acpa-cpf.org/wpontent/uploads/2017/06/Parameters_
Rev_2009_9_.pdf
5. Jugessur A., Shi M., Gjessing H.K., et al. Fetal genetic risk of
isolated cleft lip only (CLO) versus isolated cleft lip and palate (CLP): A
sub-phenotype analysis using two population-based studies of orofacial
clefts in Scandinavia // Birth Defects Res A Clin. Mol. Teratol. - 2011. - V.91
(2). - P. 85-92.
6. Mai CT, Isenburg JL, Canfield MA, Meyer RE, Correa A,
Alverson CJ, Lupo PJ, Riehle-Colarusso T, Cho SJ, Aggarwal D, Kirby
RS. Национальные популяционные оценки основных врожденных

International Journal of Scientific Pediatrics
May 2022 / Issue 01 / Article 03
29
published: 31 May 2022
дефектов, 2010–2014 гг. Исследование врожденных дефектов. 2019;
111(18): 1420-1435.
7. McGinniss M. J., Kazazian H. H., Hoyer L. W., Bi L., Inaba H.,
Antonarakis S. E. Spectrum of mutations in CRM-positive and CRM-
reduced hemophilia A. Genomics 15: 392- 398, 1993. PMID: 8449505.
8. McVey J. H., Rallapalli P. M., Kemball-Cook G., et al. The European
Association for Haemophilia and Allied Disorders (EAHAD) Coagulation
Factor Variant Databases: Important resources for haemostasis clinicians
and researchers. Haemophilia. 2020; 26: 306– 313. PMID: 32166871
9. “Peyvandi F., Garagiola I. Clinical advances in gene therapy
updates on clinical trials of gene therapy in haemophilia. Haemophilia.
2019 Sep;25(5):738-746. doi: 10.1111/hae.13816. Epub 2019 Jul 8. PMID:
31282050.
10. Nathwani A. C., Davidoff A. M., Tuddenham E. G. D. Advances
in Gene Therapy for Hemophilia. Hum Gene Ther. 2017 Nov;28(11):1004-
1012. doi: 10.1089/hum.2017.167. PMID: 28835123
11. Sherief, L.M., Gaber, O.A., Youssef, H.M. et al. Развитие
ингибитора фактора VIII у пациентов с египетской гемофилией: играет
ли роль мутация инверсии интрона 22. Ital J. Pediatr 46, 129 (2020).
https://doi.org/10.1186/s13052-020-00878-5
12. Whittaker D L, D L Copeland, J B Graham. Linkage of color
blindness to hemophilias A and B. Am J Hum Genet 1962 Jun;14(2):149-
58. PMID: 14006651 PMCID: PMC1932287





