





- 152 -
7. Якубов Р.К., Шарипова А.У.,Якубов
Р.Р.Развитие деформаций челюстей и их
осложнений у детей с первично-костными
заболеваниями и повреждениями ВНЧС.
Причинно-следственная связь//
Stomatologiya. –2009. - № 1-2 (39-40). -С.58-
61.
8.Якубов Р.К.,Азимов М.И Результаты
комплексного обследования детей с
вторичным деформирующими остеоартрозом
ВНЧС// Стоматология. –2001. №5. –С.37-39.
9
.
Якубов Р.К., Азимов М.И.,
Досмухамедова Д.3. и др. Методы
комплексного лечения и реабилитации детей с
приобретенными дефектами и деформациями
зубочелюстной системы: Метод.
рекомендации. - Ташкент, 1999. - 18 с.
Оценка состояния челюстно-лицевой области
у женщин, родивших детей с врожденной
дисплазией костной системы.
Якубов Р.К., Нигматов Р.Н., Якубова Н.А.
В статье представлены результаты
обследования 30 матерей детей с вторич-
ным деформирующим остеоартрозом,
врожденными аномалиями височно-нижне-
челюстного сустава, хроническим
деструктивным остеомиелитом . Выявлены
идентичные проявления патологии
зубочелюстной системы, жалобы и и
признаки патологии внутренних органов и
систем. Авторы обосновывают
необходимость проведения комплексного
обследования .
SUMMARY
ESTIMATION OF СОNDITION OF
MAXILLOFACIAL AREAS AT THE WOMEN
WHO HAVE GIVEN BIRTH TO CHILDREN
WITH A CONGENITAL DYSPLASIA OF
OSTEAL SYSTEM
Yakubov R. K, Nigmatov R. N. Yakubova
N.A.
In results of inspection of 30 mothers of
children are presented article with a secondary
deforming osteoarthrosis, congenital anomalies
temporally
-
m
andibular
joint,
a
chronic
destructive osteomyelitis. Are taped
i
dentical
implications of a pathology of dentoalveolar
system, the complaint and signs
p
athologies of
internal organs and systems. Authors prove
necessity of carrying out of complex inspection.
Surgical Strategies
in Severely Atrophic Posterior Mandible & Maxilla
Ho Kyun Seo, DDS
Director, Hyung Dental Clinic (Private Practice), Seoul, Korea
Clinical Associate Professor, Medical School, Ewha Women’s University
In case of severely atrophic alveolar ridge
in posterior area of mandible and maxilla, Ridge
Augmentation with bone graft, Distraction
Osteogenesis, Implantation with short and wide
Implant,
Inferior
Alveolar
Nerve
Transpositioning, Bypass mandibular canal is
possible for implant restoration.
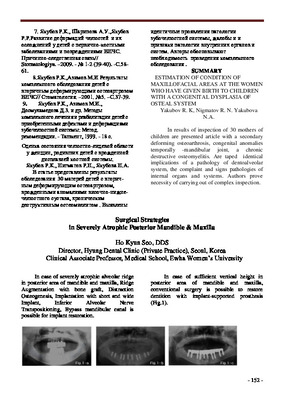
In case of sufficient vertical height in
posterior area of mandible and maxilla,
conventional surgery is possible to restore
dentition with implant-supported prosthesis
(Fig.1).

[Введите название документа]
But conventional implant surgery is
impossible in case of severely atrophic posterior
area. 4 or 6 implants can be installed at
interforaminal area (anterior area of both mental
foramens) instead of implant installation at
posterior area. And magnetic overdenture can be
fabricated (Fig.2).
It is mandatory to install implants in
posterior area for fixed-type implant-supported
prosthesis even if advanced alveolar bone
resorption occured. Implantation with short and
wide-diameter implant, Inferior Alveolar Nerve
Transpositioning, Bypass mandibular canal is
discussed to restore posterior dentition with
fixed-type implant-supported prosthesis.
Facial
neurosensory
dysfunction
by
mandibular nerve damage can be happened
during implant surgery at posterior area of
mandible. So neurosensory dysfunction test is
mentioned prior to discuss the surgical
maneuvers. Light Touch (LT) Test and Brush
Stroke Direction (BSD) test is performed with
soft feather or brush. The test result of sense and
sensibility at affected side is compared with
contra-lateral side. 2 sharp explorers are used to
distinguish the two different points in Two-Point
Discrimination (2-P) Test.
1. Inferior Alveolar Nerve Transpositioning
51 year-old female patient came for
implant restoration. She had Upper complete
denture and lower removable partial denture.
Advanced periodontitis could be observed
around lower left 2
nd
premolar (Fig.3). Patient is
sensitive to percussion and had discomfort to
wear and remove lower denture. Tooth mobility
is severe and pus discharge was observed from
the gingival sulcus. Large radiolucency was seen
in standard dental x-ray.
She didn’t want to use lower denture and
to make new denture neither. She wanted
implant installation and fixed-type prosthesis. To
satisfy the patient’s demand, implant should be
installed in atrophic posterior area. Possible
treatment options were suggested to the patient.
And the patient decided implant installation with
nerve transpositioning. Longer implants were
installed and excellent initial stability could be
achieved
(Fig.4).
Patient
had
transient
parasthesia immediately after surgery but it did
not interrupt patient’s normal function.
Preoperative instruction was helpful for the
patient understand and adapt to postoperative
condition. 5-year-postoperative follow-up was
performed. Installed implants, prosthesis, and
surrounding periodontal tissue is stable and the
patient satisfies the treatment results (Fig.5).

[Введите название документа]
2. Use of Wide & Short Implant
Gravesetal and Davarpanahetal et al.
reported that the success rate of wide-diameter
implant is 95.9% and 96.3%. And multicenter
study of Nobel Biocare reported the 97.9%
success rate of wide-diameter implant. Wide-
diameter implant can be installed in atrophic
maxillary posterior area without additional
surgical intervention such as maxillary sinus
lifting
and
in
mandible
without
nerve
transpositioning. And it can also suggest
sufficient platform surface between implant
fixture and prosthesis that can reduce the
possibility of screw loosening, screw and/or
fixture fracture. Wide-diameter implant can
suggest more biologic emergency profile. So
more esthetic prosthesis can be fabricated and
surrounding periodontium is stabilized for long
time.
1) Wide-diameter implant can be installed
only with simple GBR around fixture in
mandible
without
additional
surgical
intervention such as nerve repositioning or ridge
augmentation (Fig.6).
2) Conventional maxillary sinus lifting is
not needed in atrophic maxillary posterior area
so that healing period and patient’s discomfort
can
be
minimized
(Fig.7).

- 155 -
3) Wide-diameter implant can be simply
installed in case of large bony defect such as
molar extraction site. Sufficient initial stability
can be achieved and rapid soft tissue healing is
expected. Need for socket preservation,
prolonged healing period of extraction socket is
not acquired (Fig.8).
And the quantity of bone graft, possibility
of additional soft tissue management is reduced
in large bony defect (Fig.9).
4) In case of failed implant removal and
reinstallation of fixture, wide-diameter implant
is useful to achieve initial stability and simple
and better surgical result (Fig.10).
3. Bypass Mandibular Canal
Some patient has severely atrophic
mandible not to install short and wide-diameter
implant. In case of severely atrophic mandible,
Implant can be installed lateral to mandibular
canal to bypass it. Anatomically, mandibular
neurovascular bundle pass mandibular canal
through mandibular foramen on medial (inner)
side of ramus of mandible and goes out through
mental foramen on lateral (outer) side of
mandibular div. Although posterior alveolar
ridge of mandible is severely resorbed, the space
that implant can be installed into is possibly
available at lateral side to mandibular canal
(Fig.11).

- 156 -
68-year-old female patient had severely
resorbed alveolar ridge due to using upper and
lower complete denture over 30 years. She
complained insufficient retention and pain
during mastication and speaking. She wanted
fixed-type implant supported prosthesis. 6
implants were installed in interforaminal area
and 2 short and wide-diameter implants were
installed in lateral side to mandibular canal to
bypass it (Fig.12-14).
After the surgery, patient had no
abnormality on neurosensory dysfunction test.
She didn’t complain motor and sensory
dysfunction to interrupt normal function. Rapid
intra-oral soft tissue healing was observed.
Uncovering was performed about 10 weeks after
1
st
surgery and provisional fixed-type prosthesis
was set. Secondary stability at 2
nd
surgery was
good. Significant improvement of mastication
and patient’s comfort is observed (Fig.15-16).

- 157 -
ОПЫТ ПРИМЕНЕНИЯ ДЕНТАЛЬНЫХ СУБПЕРИОСТАЛЬНЫХ ИМПЛАНТАНТОВ ИЗ
СПЛАВА ВИТАЛЛИУМА
Алымбаев Р.С.
Кыргызская государственная медицинская академия, Бишкек, Кыргызская республика
Одной из главных проблем современной
имплантологии
сегодня
является
приобретенный дефицит костной ткани в
боковых участках челюстей вследствие
атрофических и воспалительных процессов
[1]. По данным ряда авторов, это встречается
у 29-35% пациентов, обращающихся за
имплантологической помощью. Кроме того,
от
26%
до
47%
пациентов
имеют
неблагоприятное
с
имплантологической
точки зрения морфологическое строение
челюстной
кости
(тип
костной
архитектоники по В.П. Параскевичу). У
данного контингента больных при наличии
достаточного объема кости до введения
имплантата шансы на их полноценную
биоинтеграцию
и
длительное
функционирование сомнительны [2,3].
Отдельную группу риска составляют
больные с патологическими рефлексами
(бруксизм), гиперфункцией жевательной
мускулатуры
и
тяжелой
врожденной
патологией прикуса.
Таким образом, у существенной части
больных,
нуждающихся
в
дентальной
имплантации, отсутствуют условия для
установки внутрикостных конструкций или
показания к их применению.
В настоящее время разработан ряд
методик,
обеспечивающих
возможность
введения
внутрикостных
опор
в
вышеперечисленных ситуациях: синус –
лифтинг, ауто- и аллопластика альвеолярного
отростка, направленная регенерация костной
ткани, транспозиция нижнеальвеолярного
нерва, установка имплантатов вестибулярию
и язычно от нижнечелюстного канала, а
также в бугор, скуловой и небные отростки
верхней челюсти. Все эти манипуляции, в
большей или меньшей степени технически
сложны, многоэтапны и могут вызвать
достаточно серьезные осложнения. При
проведении аутопластики альвеолярного
отростка вероятна резорбция пересаженного
материала и смещение его за счет
сокращения щечных мышц, т.к. последние
при выраженной атрофии нижней челюсти
прикрепляются рядом с вершиной гребня.
При транспозиции нижнечелюстного нерва
может
возникнуть
стойкое
нарушение
чувствительности
в
зоне
иннервации
n.alveolaris inferior, что дает повод для
сомнений в целесообразности этой операции.
При установке имплантатов в «обход»
верхнечелюстной пазухи и нижнечелюстного
канала конструкции располагаются под