Library search
Search Results
-
 IMPROVED MODEL OF METHODOLOGY FOR DEVELOPING STUDENTS' COMMUNICATIVE COMPETENCEIn this article, the relevance of the development of communicative competence of students on the basis of innovative approaches, the importance of communicativity in personality maturation, theoretical foundations of communicative competence, requirements for a modern teacher, ensuring the achievement of the development of communicative abilities through the use of effective methods in the educational process, developing and introducing effective methodologies based on, information and recommendations have been made regarding the search for new strategies to increase communicativity.
IMPROVED MODEL OF METHODOLOGY FOR DEVELOPING STUDENTS' COMMUNICATIVE COMPETENCEIn this article, the relevance of the development of communicative competence of students on the basis of innovative approaches, the importance of communicativity in personality maturation, theoretical foundations of communicative competence, requirements for a modern teacher, ensuring the achievement of the development of communicative abilities through the use of effective methods in the educational process, developing and introducing effective methodologies based on, information and recommendations have been made regarding the search for new strategies to increase communicativity.
Modern Science and Research -
 Роль зелёной экономики в формировании бизнес-модели устойчивого развитияСтатья рассматривает роль зелёной экономики в формировании бизнес-модели устойчивого развития. В контексте изменения климата и растущего сознания о необходимости охраны окружающей среды, зелёная экономика становится всё более важной для бизнеса. В статье анализируются преимущества и вызовы, связанные с внедрением зелёной экономики в бизнес-модель, а также предлагаются практические рекомендации для компаний, желающих стать устойчивыми и основать свою бизнес-модель на принципах зелёной экономики.
Роль зелёной экономики в формировании бизнес-модели устойчивого развитияСтатья рассматривает роль зелёной экономики в формировании бизнес-модели устойчивого развития. В контексте изменения климата и растущего сознания о необходимости охраны окружающей среды, зелёная экономика становится всё более важной для бизнеса. В статье анализируются преимущества и вызовы, связанные с внедрением зелёной экономики в бизнес-модель, а также предлагаются практические рекомендации для компаний, желающих стать устойчивыми и основать свою бизнес-модель на принципах зелёной экономики.
Modern Science and Research -
 Assessment of the level of organotropic autoantibodies in newborns with low body weight dies in newborns with low body weight
Assessment of the level of organotropic autoantibodies in newborns with low body weight dies in newborns with low body weight
in LibraryThe frequency of preterm birth is variable, but in most developed countries in recent decades it has been quite stable and amounts to 5-10% of the number of children born[18,29,35]. The frequency of adverse outcomes among surviving children born before 28 weeks of gestation reaches 40–50%, rising to 70–90% for children weighing 500.0–750.0 g[30,32,34,36]. In children born with low body weight, mortality reaches 30% [8,30]. The current level of development of perinatology makes it possible to increase the survival of these children, but the peculiarities of their subsequent growth and development require no less attention. [8]. The fact of premature birth of children in women with a burdened obstetric-gynecological and somatic history is associated with perinatal CNS damage and often with a change in the vegetative status of a child in the first years of life. [9,37,41]. In early childhood and in subsequent periods of development, these children show psychosomatic abnormalities, in particular nocturnal enuresis, prolonged low-grade fever, tics and obsessive movements, attention deficit hyperactivity disorder, tension
cephalalgia, arterial hypertension, arterial hypotension, biliary dyskinesia, bronchial asthma, atopic dermatitis[27,39]. An inverse relationship has been shown between low birth weight and adult blood pressure levels, the likelihood of developing type 2 diabetes, cardiovascular disease, and an excessive response to stress [26,38]. Lack of motor development in children at 16 years of age is associated with body weight less than 2 kg at birth. [31]. IQ tests showed that 41% of children born at the 7th month of pregnancy had worse performance compared to their healthy peers and had learning problems [41]. Early preterm birth can negatively affect puberty and increase the chance of adolescent depression [16], as these children may slow down the process of myelination of the frontal lobe of the brain, which is responsible for motivation, satisfaction, short-term memory and vision. [35]. Studies conducted among adolescents born prematurely revealed anomalies in their brain development, namely, a lack of gray matter in the temporal brain and cerebellum [37]. -
 Данная статья посвящена изучению возникновения и развития эпистолярия. В статье представлен краткий обзор истории возникновения и развития эпистолярия, проанализированы и систематизированы научные подходы ученых относительно определения данного понятия и определены основные классификации эпистолярных текстов.
Данная статья посвящена изучению возникновения и развития эпистолярия. В статье представлен краткий обзор истории возникновения и развития эпистолярия, проанализированы и систематизированы научные подходы ученых относительно определения данного понятия и определены основные классификации эпистолярных текстов. -
 Ensuring sustainable economic development of industrial enterprises in the world pandemic
Ensuring sustainable economic development of industrial enterprises in the world pandemic
Economics and innovative technologiesThe article examines the problems of sustainable development of industrial enterprises, analyzes the factors affecting the sustainability of enterprise development, gives a definition of various types of economic sustainability during a pandemic, and highlights the internal and external factors of the sustainability of enterprises. It is shown that of the most
important factors affecting the sustainability of the development of industrial enterprises, first of all, economic stability stands out. The factors in the conditions of a deteriorating economic situation are investigated and identified, which are advisable to take into account when solving the problem of sustainable development of industrial enterprises. When conducting the study, the main sources of data were the materials of state statistics committee of the Republic of Uzbekistan. The methodological developments are based on comparative methods of analysis. Proposals have been developed to ensure economic sustainable development of industrial enterprises during a pandemic. -
 Frequency of occurrence small anomalies of development in children in the region PriaralyaWe examined 988 children aged from 3 till 6 years living in the Khorezm area and control group of 150 children of of Tashkent. The following methods were applied to inspection of children: kliniko-anamnesticheskiya, according to the analysis of fizikalny survey and primary medical documentation, and also instumentalny methods of research. By results of our research small anomalies of development and congenital defects of bodies and systems vyyavlit at children in ecologically unsuccessful regions by 3 times more often than at their contemporaries in ecologically safe region, a thorax and a backbone (50,3%) are characterized by the high frequency of combinations various the fenotipicheskikh and congenital morphogenetic options of development of skin (96,2%), the sky (81,6%), extremities and joints (77,5%).
Frequency of occurrence small anomalies of development in children in the region PriaralyaWe examined 988 children aged from 3 till 6 years living in the Khorezm area and control group of 150 children of of Tashkent. The following methods were applied to inspection of children: kliniko-anamnesticheskiya, according to the analysis of fizikalny survey and primary medical documentation, and also instumentalny methods of research. By results of our research small anomalies of development and congenital defects of bodies and systems vyyavlit at children in ecologically unsuccessful regions by 3 times more often than at their contemporaries in ecologically safe region, a thorax and a backbone (50,3%) are characterized by the high frequency of combinations various the fenotipicheskikh and congenital morphogenetic options of development of skin (96,2%), the sky (81,6%), extremities and joints (77,5%).
Doctor's Herald -
 Использование 3-д моделирования для оказания дистанционной первой ортодонтической и ортопедической помощи детям с врожденной расщелиной верхней губы и нёба
Использование 3-д моделирования для оказания дистанционной первой ортодонтической и ортопедической помощи детям с врожденной расщелиной верхней губы и нёба
Topical issues of surgical dentistry and dental implantologyВрождённая расщелина губы и нёба относятся к порокам развития, которые вызывают аномалии общей костной системы, пороки развития челюстнолицевого скелета и зубной дуги, аномалии мышечной системы. Расщелины губы и нёба могут нарушать функции сосания, глотания и дыхания у новорожденных. Так же возможны вторичные зубочелюстные аномалии, связанные с патологическим воздействием языка на альвеолярный отросток нижней челюсти. Поэтому медицинскую реабилитацию детей с врожденной аномалией следует начинать как можно раньше. Необходимо разделить ротовую и носовую полости, чтобы восстановить физиологические функции питания и дыхания. Также важно восстановить форму альвеолярных отростков, нарушенную врожденной патологией.
-
 ACCOMPANYING DEFECTS OF DEVELOPMENT IN CHILDREN WITH CONGENITAL CLEFT OF LIP AND PALATEAn analysis of the treatment of 122 patients with various types of congenital clefts of the upper lip and palate was performed on the basis of the 2nd clinic of the Samarkand State Medical Institute. As a result of our studies, it was found that congenital clefts of the upper lip and palate are found in combination with developmental abnormalities of other organs. The main ones were short frenulum of lips and tongue in 76 patients, low body mass index in 97, vertebral deformity in 6, clubfoot in 19, congenital flat feet in 5, congenital dysplasia of the hip joint in 2, defects in the development of the urinary system in 19, prenatal encephalopathy in 46, congenital muscle failure in 15 children. Analysis of the study showed that to achieve a high level of medical care for children with this pathology, a clear and uniform, interconnected tactics of all specialists involved in the treatment of a child with congenital cleft lip and palate is required.
ACCOMPANYING DEFECTS OF DEVELOPMENT IN CHILDREN WITH CONGENITAL CLEFT OF LIP AND PALATEAn analysis of the treatment of 122 patients with various types of congenital clefts of the upper lip and palate was performed on the basis of the 2nd clinic of the Samarkand State Medical Institute. As a result of our studies, it was found that congenital clefts of the upper lip and palate are found in combination with developmental abnormalities of other organs. The main ones were short frenulum of lips and tongue in 76 patients, low body mass index in 97, vertebral deformity in 6, clubfoot in 19, congenital flat feet in 5, congenital dysplasia of the hip joint in 2, defects in the development of the urinary system in 19, prenatal encephalopathy in 46, congenital muscle failure in 15 children. Analysis of the study showed that to achieve a high level of medical care for children with this pathology, a clear and uniform, interconnected tactics of all specialists involved in the treatment of a child with congenital cleft lip and palate is required.
Journal of oral medicine and craniofacial research -
 FREQUENCY OF MEETING ANORECTAL MALFORMATION AT ANTENATAL DIAGNOSTICS IN CHILDREN OF SAMARKAND AND SAMARKAND REGION1 he prevalence ot anorectal malformations ranges from I: JJUO to I: 5000 cases ot live births. With the development of antenatal diagnosis, ultrasound criteria specific to anus atresia are currently being actively discussed. The most affordable and effective method that allows you to establish anorectal malformations during pregnancy is ultrasound of the fetus. According to the approved protocol, when a fetus reveals sonographic signs of malformation in a screening center, the pregnant woman attaches herself to the department of pregnancy pathology. Screening ultrasound examination of pregnant women was performed at gestational age 20-22 weeks. Thus, antenatal ultrasound performed during gestational periods of 20-22 weeks shows a rather high information content for identifying sonographic signs, especially without fistulous forms of AWP in the fetus with a sensitivity of 57.1%. specificity - 98.8% and overall accuracy - 96.5 %.
FREQUENCY OF MEETING ANORECTAL MALFORMATION AT ANTENATAL DIAGNOSTICS IN CHILDREN OF SAMARKAND AND SAMARKAND REGION1 he prevalence ot anorectal malformations ranges from I: JJUO to I: 5000 cases ot live births. With the development of antenatal diagnosis, ultrasound criteria specific to anus atresia are currently being actively discussed. The most affordable and effective method that allows you to establish anorectal malformations during pregnancy is ultrasound of the fetus. According to the approved protocol, when a fetus reveals sonographic signs of malformation in a screening center, the pregnant woman attaches herself to the department of pregnancy pathology. Screening ultrasound examination of pregnant women was performed at gestational age 20-22 weeks. Thus, antenatal ultrasound performed during gestational periods of 20-22 weeks shows a rather high information content for identifying sonographic signs, especially without fistulous forms of AWP in the fetus with a sensitivity of 57.1%. specificity - 98.8% and overall accuracy - 96.5 %.
Doctor's Herald -
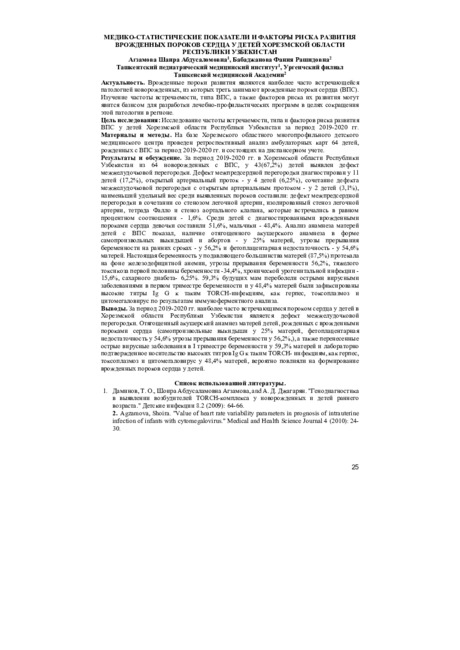 Медико-статистические показатели и факторы риска развития врожденных пороков сердца у детей Хорезмской области Республики УзбекистанВрожденные пороки развития являются наиболее часто встречающейся патологией новорожденных, из которых треть занимают врожденные пороки сердца (ВПС). Изучение частоты встречаемости, типа ВПС, а также факторов риска их развития могут явится базисом для разработки лечебно-профилактических программ в целях сокращения этой патологии в регионе.
Медико-статистические показатели и факторы риска развития врожденных пороков сердца у детей Хорезмской области Республики УзбекистанВрожденные пороки развития являются наиболее часто встречающейся патологией новорожденных, из которых треть занимают врожденные пороки сердца (ВПС). Изучение частоты встречаемости, типа ВПС, а также факторов риска их развития могут явится базисом для разработки лечебно-профилактических программ в целях сокращения этой патологии в регионе.
Инновационные подходы к диагностике, лечению и профилактике туберкулеза и неспецефической респираторной патологии у взрослых и детей -
 The article examines the current state of the real estate appraisal system in our country. Existing problems in the property valuation process and their impact on property relations were assessed. Opportunities to optimize the process of reforming the property system in the context of modern market relations have been studied. In the process of improving the system of property reform in Uzbekistan is based on the possibility of adapting the process of real estate appraisal to the requirements of the property market. Scientific proposals and practical recommendations for improving the effectiveness of property reforms by improving the system of real estate valuation have been formed.
The article examines the current state of the real estate appraisal system in our country. Existing problems in the property valuation process and their impact on property relations were assessed. Opportunities to optimize the process of reforming the property system in the context of modern market relations have been studied. In the process of improving the system of property reform in Uzbekistan is based on the possibility of adapting the process of real estate appraisal to the requirements of the property market. Scientific proposals and practical recommendations for improving the effectiveness of property reforms by improving the system of real estate valuation have been formed. -
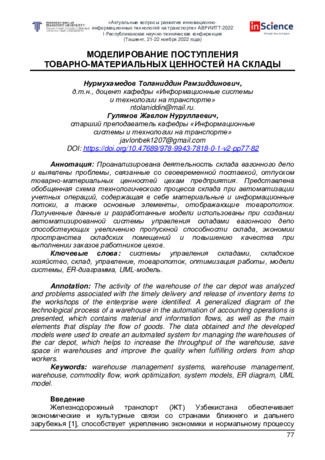 Modeling the receipt of inventory items at warehouses
Modeling the receipt of inventory items at warehouses
Current issues of development of innovative and information technologies in transportThe activity of the warehouse of the car depot was analyzed and problems associated with the timely delivery and release of inventory items to the workshops of the enterprise were identified. A generalized diagram of the technological process of a warehouse in the automation of accounting operations is presented, which contains material and information flows, as well as the main elements that display the flow of goods. The data obtained and the developed models were used to create an automated system for managing the warehouses of the car depot, which helps to increase the throughput of the warehouse, save space in warehouses and improve the quality when fulfilling orders from shop workers.
-
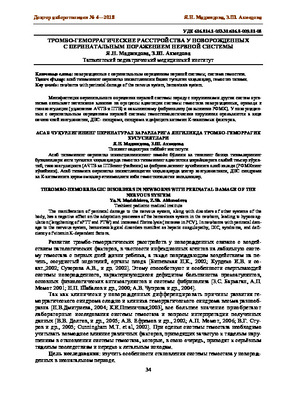 Thrombo-hemorrhagic disorders in newborns with perinatal damage of the nervous systemThe manifestation of perinatal damage to the nervous system, along with disorders of other systems of the body, has a negative effect on the adaptation processes of the hemostasis system in the newborn, leading to hypocoagulation (lengthening of aPTT and PTW) and increased fibrinolysis (increase in PCV). In newborns with perinatal damage to the nervous system, hemostasiological disorders manifest as hepatic coagulopathy, D1C, syndrome, and deficiency of vitamin К-dependent factors.
Thrombo-hemorrhagic disorders in newborns with perinatal damage of the nervous systemThe manifestation of perinatal damage to the nervous system, along with disorders of other systems of the body, has a negative effect on the adaptation processes of the hemostasis system in the newborn, leading to hypocoagulation (lengthening of aPTT and PTW) and increased fibrinolysis (increase in PCV). In newborns with perinatal damage to the nervous system, hemostasiological disorders manifest as hepatic coagulopathy, D1C, syndrome, and deficiency of vitamin К-dependent factors.
Doctor's Herald -
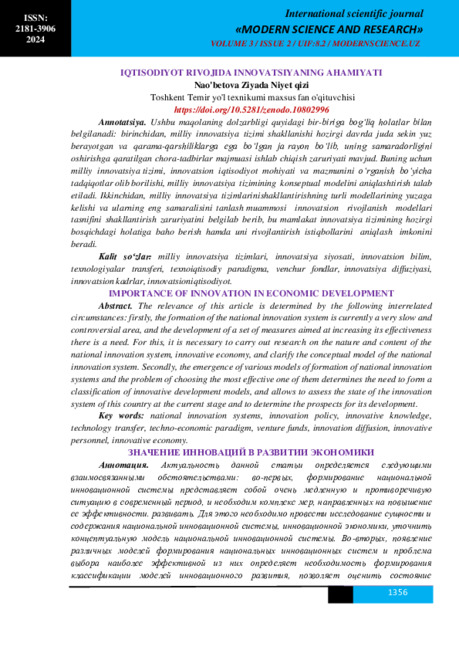 The relevance of this article is determined by the following interrelated circumstances: firstly, the formation of the national innovation system is currently a very slow and controversial area, and the development of a set of measures aimed at increasing its effectiveness there is a need. For this, it is necessary to carry out research on the nature and content of the national innovation system, innovative economy, and clarify the conceptual model of the national innovation system. Secondly, the emergence of various models of formation of national innovation systems and the problem of choosing the most effective one of them determines the need to form a classification of innovative development models, and allows to assess the state of the innovation system of this country at the current stage and to determine the prospects for its development.
The relevance of this article is determined by the following interrelated circumstances: firstly, the formation of the national innovation system is currently a very slow and controversial area, and the development of a set of measures aimed at increasing its effectiveness there is a need. For this, it is necessary to carry out research on the nature and content of the national innovation system, innovative economy, and clarify the conceptual model of the national innovation system. Secondly, the emergence of various models of formation of national innovation systems and the problem of choosing the most effective one of them determines the need to form a classification of innovative development models, and allows to assess the state of the innovation system of this country at the current stage and to determine the prospects for its development. -
 Effective organization of management in the further development of the tax system of UzbekistanRole of management in further rationalizing and advancing of tax system of Republic Uzbekistan, comparative analysis of significant advancing in structural organization of administrative bodies of tax system between 2000 year and nowadays, and information on calculation of average quantity of workload of employee of tax service in relative order was lightened up in this article.
Effective organization of management in the further development of the tax system of UzbekistanRole of management in further rationalizing and advancing of tax system of Republic Uzbekistan, comparative analysis of significant advancing in structural organization of administrative bodies of tax system between 2000 year and nowadays, and information on calculation of average quantity of workload of employee of tax service in relative order was lightened up in this article.
Economics and innovative technologies -
 The article examines the current state of the real estate appraisal system in our country. Existing problems in the property valuation process and their impact on property relations were assessed. Opportunities to optimize the process of reforming the property system in the context of modern market relations have been studied. In the process of improving the system of property reform in Uzbekistan is based on the possibility of adapting the process of real estate appraisal to the requirements of the property market. Scientific proposals and practical recommendations for improving the effectiveness of property reforms by improving the system of real estate valuation have been formed
The article examines the current state of the real estate appraisal system in our country. Existing problems in the property valuation process and their impact on property relations were assessed. Opportunities to optimize the process of reforming the property system in the context of modern market relations have been studied. In the process of improving the system of property reform in Uzbekistan is based on the possibility of adapting the process of real estate appraisal to the requirements of the property market. Scientific proposals and practical recommendations for improving the effectiveness of property reforms by improving the system of real estate valuation have been formed -
 THE EFFECTIVENESS TREATMENT OF DISTAL OCCLUSION PATHOLOGY USING A MODIFIED TWIN-BLOCK DEVICEDistal occlusion is one of the most common forms of dentoalveolar anomalies, accompanied by functional changes in the masticatory muscles. In addition, in adult patients, distal occlusion, as a rule, is combined with defects in the dentition. The issues of diagnosis and treatment of patients with distal occlusion in combination with pathology of the masticatory muscles have always received great attention. Orthodontic treatment is based on the timely diagnosis of early forms of anomalies to prevent the problem and ensure the normal development of the child's dentition. Dcntofacial anomalies are formed from subtle symptoms and, as the child grows, take the form of a complex formed anomaly, which requires many years of laborious and expensive orthodontic treatment. Providing conditions for the harmonious growth and development of the child is the main task in pediatric dentistry. Functional devices that affect the change in the growth of the jaws, the muscular environment of the dental arches, play an important role in the treatment of dentoalveolar anomalies. In recent years, with the development of the functional direction in the treatment of dentoalveolar anomalies, new standard functional devices have appeared - trainers, LM activators, myobraces. These devices allow you to normalize the position of the teeth and contribute to the early correction of dental anomalies. Functional devices train the muscles of the maxillofacial region, contribute to the normalization of the functions of the dentoalveolar system, and optimize the formation of thedentoalveolar system during the growth and development of the jaws. All this, in turn, ensures the stability of treatment results. The Clarke twin-block is used for the correction of class II and III occlusion, the normalization of the functions of the dentition.
THE EFFECTIVENESS TREATMENT OF DISTAL OCCLUSION PATHOLOGY USING A MODIFIED TWIN-BLOCK DEVICEDistal occlusion is one of the most common forms of dentoalveolar anomalies, accompanied by functional changes in the masticatory muscles. In addition, in adult patients, distal occlusion, as a rule, is combined with defects in the dentition. The issues of diagnosis and treatment of patients with distal occlusion in combination with pathology of the masticatory muscles have always received great attention. Orthodontic treatment is based on the timely diagnosis of early forms of anomalies to prevent the problem and ensure the normal development of the child's dentition. Dcntofacial anomalies are formed from subtle symptoms and, as the child grows, take the form of a complex formed anomaly, which requires many years of laborious and expensive orthodontic treatment. Providing conditions for the harmonious growth and development of the child is the main task in pediatric dentistry. Functional devices that affect the change in the growth of the jaws, the muscular environment of the dental arches, play an important role in the treatment of dentoalveolar anomalies. In recent years, with the development of the functional direction in the treatment of dentoalveolar anomalies, new standard functional devices have appeared - trainers, LM activators, myobraces. These devices allow you to normalize the position of the teeth and contribute to the early correction of dental anomalies. Functional devices train the muscles of the maxillofacial region, contribute to the normalization of the functions of the dentoalveolar system, and optimize the formation of thedentoalveolar system during the growth and development of the jaws. All this, in turn, ensures the stability of treatment results. The Clarke twin-block is used for the correction of class II and III occlusion, the normalization of the functions of the dentition.
Medicine and innovations -
 Chronic pain syndrome in diseases of the peripheral nervous systemWe have examined 146 patients, 71 patients with radiculopathy, 20 with plexopathy, 23 with compres- sion-ischemic neuropathies, 32 with chronic diabetic polyneuropathy. For this study we used the following methods: MRI, CT, X-ray, DN 4 questionnaire, electroneuromyography, Spielberger–Khanin questionnaire, Montgomery-Asberg depression rating scale, asthenia scale (MFI-20). The study showed that the clinical pic-ture, narure and severity of chronic pain syndrome in diseases of the peripheral nervous system does not di- rectly depend on the degree of damage to the peripheral nerves, being determined by the degree of central mechanisms of somatosensory system regulation involvement in the pathological process
Chronic pain syndrome in diseases of the peripheral nervous systemWe have examined 146 patients, 71 patients with radiculopathy, 20 with plexopathy, 23 with compres- sion-ischemic neuropathies, 32 with chronic diabetic polyneuropathy. For this study we used the following methods: MRI, CT, X-ray, DN 4 questionnaire, electroneuromyography, Spielberger–Khanin questionnaire, Montgomery-Asberg depression rating scale, asthenia scale (MFI-20). The study showed that the clinical pic-ture, narure and severity of chronic pain syndrome in diseases of the peripheral nervous system does not di- rectly depend on the degree of damage to the peripheral nerves, being determined by the degree of central mechanisms of somatosensory system regulation involvement in the pathological process
Journal problems of biology and medicine -
 THE EFFECT OF THE DEVELOPMENT OF THE BANKING SYSTEM ON THE DEVELOPMENT OF THE NATIONAL ECONOMYThis thesis discusses the importance of developing the banking system for the formation and strengthening of the competitiveness of the economy. Various aspects of banks' impact on the economy are examined, such as financing, supporting small and medium-sized businesses, ensuring financial stability, and influencing international trade. The work also emphasizes the need for regulation and control to manage the risks associated with the development of the banking system, and provides examples from the studies of scholars studying the impact of banks on economic growth and competitiveness.
THE EFFECT OF THE DEVELOPMENT OF THE BANKING SYSTEM ON THE DEVELOPMENT OF THE NATIONAL ECONOMYThis thesis discusses the importance of developing the banking system for the formation and strengthening of the competitiveness of the economy. Various aspects of banks' impact on the economy are examined, such as financing, supporting small and medium-sized businesses, ensuring financial stability, and influencing international trade. The work also emphasizes the need for regulation and control to manage the risks associated with the development of the banking system, and provides examples from the studies of scholars studying the impact of banks on economic growth and competitiveness.
Modern Science and Research -
 Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Catalog of abstractsRelevance of the problem.Despite the great successes of angiosurgery, the problem of surgical treatment of abdominal aortic aneurysms does not lose its relevance. World health statistics records a steady increase in the incidence of abdominal aortic aneurysm (ABA). According to L.J. Melton et al. (1984) and L.K. Bickerstaff et al. (1984) in the USA the number of patients with abdominal aortic aneurysm has increased 7 times in 30 years since 1951. In England and Wales, according to F.G. Fowkers et al. (1989) for the same period revealed a 20-fold increase in abdominal aortic aneurysms in men and 11-fold in women. According to the results of multicentre screening studies ABA was detected in 8% of the examined (E.S. Vourvouri, 2001), and in the age group of 64-69 years ABA was detected in 5.7% of the examined, and in the age group of 75-81 years - in 8.9% (R.A.P. Skott et al., 2001). A similar trend is observed in other countries. Accordingly, mortality from ABA is also increasing - aneurysm rupture in a number of countries is one of the ten most frequent causes of death among elderly and senile people (F.A. Lederle et al., 1990)
Currently, planned aneurysm resection has become a recognised standard of radical treatment of ABA patients and the number of these operations is steadily increasing. For example, about 40,000 ABA resections are performed annually in the USA (J.J. Grange et al., 1997). In Sweden during the period from 1987-89 to 1993-95 the number of ABA operations increased 5 times and currently 10 operations per 100,000 population are performed (A.Hallin et al., 2001), although this is 1.5 - 2 times less than the required number. However, postoperative lethality is still quite high and makes 5-7% (A.V.Pokrovskiy et al., 1992; Y.V.Belov et al., 1992; V.V.Vakhidov et al., 1992; A.W. Bradbury et al. Bradbury et al., 1997; A.Hallin et al., 2001).
E.W. Steyeberg et al. (1995) summarised the data of literature on 17238 ABA resection operations and gave an average mortality of 6.8%.
Multicentre studies in five major hospitals in the Netherlands found that only 74% of patients underwent ABA resection without complications; 26% had some complications, 9% of which were severe and 4.1% of which were fatal (G.J. Akkersdijk et al., 1998). Similar results were obtained in the Canadian Cooperative Study (K.W. Johnston et al., 1990). It was established that the peculiarity of complications in the majority of patients was their systemic character (L.L. Lau et al, 2001) The course of the postoperative period is most often complicated by cardiac, respiratory, renal, cerebrovascular, as well as complications associated with thrombosis and bleeding (W.E. Lloyd et al., 1996; R.D. Sayers et al., 1997; J.D. Blankenstein et al., 1998; R. Ayari et al., 1998). Ayari et al., 2001)
The undisputed leadership, without doubt, belongs to cardiac complications, the incidence of which varies from 10% to 20%. Moreover, cardiac complications account for 50-70% of total mortality. Cerebrovascular complications, although not uncommon, account for no more than 1-1.5%, but their mortality reaches 40%. Complications associated with thromboses and haemorrhages in the perioperative period reach 2-5% (M.M.Reigel et al., 1987; K.W.Johnson et al., 1990; N.Franklin et al., 1993; A.A.Milne et al., 1994).
Certainly, a large number of complications after resection of abdominal aortic aneurysms is caused by the initial severity of patients' condition, however, many unresolved tactical and technical issues of patients' preparation for the operation, stage of performance in case of combined lesions of several vascular basins play a practically significant role. Adequate management of the operation itself and the immediate postoperative period is no less important, taking into account the possibility of such dreadful complications as thrombosis and embolism, cerebral and cardiac death. Until now there is no unified complex analysis of the results of treatment of uncomplicated abdominal aortic aneurysms and, accordingly, recommendations for the prevention of possible complications.
All this determined our aim and objectives of the study.
The aim of the study is to improve the results of surgical treatment of ABA by developing an effective system for determining the main risk factors of surgical treatment and optimal surgical tactics to prevent possible complications.
Scientific novelty.For the first time a complex analysis of indications and contraindications to surgical treatment of abdominal aortic aneurysms was carried out
The most significant concomitant pathology capable to lead to formidable complications and lethality during the intervention and in the nearest postoperative period was revealed. Adequate measures of their prevention and treatment were proposed.
The algorithm of surgical treatment tactics for patients with combined pathology of coronary arteries and aortic arch branch lesions was developed
The state of haemostasis system at all stages of reconstructive surgery on abdominal aorta, starting from skin incision to wound closure, was studied for the first time.
Conclusions:
1. The proposed original classification of ABA, based on mutual dependence on the etiology of the disease, localisation, concomitant diseases, clinic and its course, allows to determine the strategy of early diagnosis, to estimate the most significant risk factors, the stage of intervention in combined lesions of adjacent and distant vascular basins and, ultimately, to determine the ways to reduce complications and mortality in patients with ABA.
2. The most informative methods of ABA diagnostics are duplex scanning and computed tomography. Non-invasive diagnostics capabilities are enough to determine the aneurysm size, its relation to the renal arteries, as well as to find out the state of visceral branches and aortic bifurcation. Abdominal aortography is indicated in patients with concomitant arterial hypertension to identify the state of the renal arteries.
3. Significant risk factors in these patients are ischaemic heart disease (44.1%), arterial hypertension (49%), haemostasis disorders (almost 100%).
4. The leading concomitant disease in the development of postoperative complications is ischaemic heart disease. Its share in abdominal aortic aneurysms is 40%. Postoperative cardiac complications reach 14.9%. Diagnostics of ischaemic heart disease should be based on the stage-by-stage detection of coronary lesions and its functional-compensatory abilities.
5. The main complications of the postoperative period after ABA resections are acute heart failure (14,9%), cerebral circulatory disorders (1,5%), acute renal failure (3,33%).
6. When significant coronary vascular channel lesions are detected in patients with ABA, it is fundamental to solve the issue of intervention staging. At 3-4 functional classes of circulatory insufficiency, appearance of new zones of hypo- or akinesia, decrease of ejection fraction below 40%, the first stage should be myocardial revascularisation surgery
7. In patients with combined lesions of brachiocephalic vessels in patients with ABA it is reasonable to assess the cerebral blood flow. In the presence of 70% or more stenosis of VCA, presence of embologenic plaque, bilateral haemodynamically significant stenosis it is necessary to perform carotid artery intervention as the first stage.
8. One of the most difficult problems of reconstructive operations in ABA is the contiguous lesion of renal and visceral branches of the abdominal aorta. The principle is their one-stage reconstruction. The types of reconstruction of these branches should be variable depending on the volume and extent of the pathological process.
9. Patients with aneurysmal lesion of abdominal aorta initially always have significant disorders of haemostasis system. In 30% of patients with occlusive diseases of aorta and its branches in the preoperative period the activity of thrombocytic-vascular link of hemostasis is increased, antithrombotic ability of vascular wall endothelium is decreased and blood rheological properties are disturbed. Activation of fibrinolysis was noted in patients with aneurysmal lesion of abdominal aorta.
10. During the operation for abdominal aortic aneurysmal lesion, after starting the blood flow the level of plasminogen increases additionally by 30%, which is a risk factor for haemorrhagic complications in the perioperative period. On the 1-3 day after the operation there is a significant decrease of blood anticoagulant potential - antithrombin-Sh by 25-27%, protein C by 23-25%. This period is the most dangerous in terms of thrombohemorrhagic complications development.
11. When using standard heparin during the operation there is a consumption of antithrombin-Sh by 30-45% and increase of platelet aggregation by 10%, which is a threatening condition for the occurrence of thrombosis of deep veins of the lower extremities with subsequent TELA. When using fraxiparin during reconstructive vascular surgeries the consumption of antithrombin-Sh and increase in platelet aggregation do not occur, prothrombin time, activated partial thromboplastin time, thrombin time are lengthened insignificantly that testifies to expediency of its use for prevention of thrombohemorrhagic complications.
12. Application of the diagnostic methods proposed by us to detect the main risk factors during the operation and in the nearest postoperative period, use of the algorithm of stage and volume of intervention allowed to reduce significantly the number of threatening complications, thus the lethality decreased 4 times, and the number of non-fatal complications - 4 times non-fatal complications - 1.5 times. -
 Conceptual foundations of economic development and the system of territorial administrationThe article economic development and regional management system. In addition, economic development, diversity management concept, the specifics of control activities have been highlighted, control systems, such as the development of mechanisms for economic issues.
Conceptual foundations of economic development and the system of territorial administrationThe article economic development and regional management system. In addition, economic development, diversity management concept, the specifics of control activities have been highlighted, control systems, such as the development of mechanisms for economic issues.
Economics and innovative technologies -
 Different approaches to creating a system of indicators of sustainable development of the tourism sectorThe article highlights the different approaches and methods for the determination of indicators of sustainable development of tourism. In particular, it deals with the idea of risk management in tourist destinations and their economic effect, which reveal the importance of risk management in the definition of sustainable development as well as creating a method of differential grouped socio-economic indicators required for the functioning of the system.
Different approaches to creating a system of indicators of sustainable development of the tourism sectorThe article highlights the different approaches and methods for the determination of indicators of sustainable development of tourism. In particular, it deals with the idea of risk management in tourist destinations and their economic effect, which reveal the importance of risk management in the definition of sustainable development as well as creating a method of differential grouped socio-economic indicators required for the functioning of the system.
Economics and innovative technologies -
Речь — важнейшая составляющая нервно-психического развития ребенка, становление которой в первые годы жизни определяет ее качество во все последующие возрастные периоды. Так, ежегодно 35–37% детей рождаются больными или заболевают в период новорожденности, не менее 9–10% детей рождаются недоношенными и с низкой массой тела [1]. Для формирования речи определяющим является период от первого года жизни до 3–5лет. Именно в это время происходит интенсивное развитие мозга и его функций.
-
 Analysis of the state of development of the transport system and assessment of its place in economic growthResearch on the analysis of the development state of transport system and estimation its role to the economic growth by using statistic methods have been made in this report. The main trends of the transport services market development cause and effect links of value – added cost formation of the freight and passenger transport have been set. Scientific recommendations on efficient use of transport potential of the economy have also been developed
Analysis of the state of development of the transport system and assessment of its place in economic growthResearch on the analysis of the development state of transport system and estimation its role to the economic growth by using statistic methods have been made in this report. The main trends of the transport services market development cause and effect links of value – added cost formation of the freight and passenger transport have been set. Scientific recommendations on efficient use of transport potential of the economy have also been developed
Economics and innovative technologies -
 SCIENTIFIC SUBSTANTIATION OF ORGANIZATIONAL APPROACHES IN THE DEVELOPMENT AND INCREASE OF COMPETITIVENESS OF THE PRIVATE SECTOR IN THE CONTEXT OF REFORMING THE HEALTH CARE SYSTEM OF THE REPUBLIC OF UZBEKISTANConduct an analysis and comparative assessment of the characteristics of the medical services market and its trends in the development of medical organizations, as well as their competitiveness in health care systems. To substantiate the modern directions of development and increasing the competitiveness of private medical organizations. To identify defects in the internal quality control system of medical care operating in private medical organizations and to develop proposals for its improvement. Analyze the organization of training and incentives for medical personnel in private medical organizations; to develop proposals for improving the intra-organizational system of continuous professional development and growth of medical personnel. Develop a comprehensive model for increasing competitiveness, introduce its basic elements into the work of private medical organizations and assess their effectiveness.
SCIENTIFIC SUBSTANTIATION OF ORGANIZATIONAL APPROACHES IN THE DEVELOPMENT AND INCREASE OF COMPETITIVENESS OF THE PRIVATE SECTOR IN THE CONTEXT OF REFORMING THE HEALTH CARE SYSTEM OF THE REPUBLIC OF UZBEKISTANConduct an analysis and comparative assessment of the characteristics of the medical services market and its trends in the development of medical organizations, as well as their competitiveness in health care systems. To substantiate the modern directions of development and increasing the competitiveness of private medical organizations. To identify defects in the internal quality control system of medical care operating in private medical organizations and to develop proposals for its improvement. Analyze the organization of training and incentives for medical personnel in private medical organizations; to develop proposals for improving the intra-organizational system of continuous professional development and growth of medical personnel. Develop a comprehensive model for increasing competitiveness, introduce its basic elements into the work of private medical organizations and assess their effectiveness.
Medicine and innovations