Library search
Search Results
-
GENETIC RISK FACTORS ASSOCIATED WITH THROMBOSIS IN A SAMPLE OF IRAQ POPULATION
The American Journal of Medical Sciences and Pharmaceutical ResearchThrombosis is a complex disorder influenced by various genetic factors. This research paper aims to investigate the genetic risk factors associated with thrombosis in a sample of the Iraq population. Understanding the genetic determinants of thrombosis is crucial for early detection, prevention, and personalized treatment strategies. This study examines a sample of the Iraq population to identify specific genetic variations and polymorphisms that may contribute to an increased risk of thrombosis. Through genetic analysis techniques, such as polymerase chain reaction (PCR) and sequencing, the study explores the prevalence and potential impact of these genetic risk factors on thrombosis. The findings provide valuable insights into the genetic underpinnings of thrombosis in the Iraq population and may have implications for risk assessment, diagnosis, and targeted interventions.
-
Risk Of Pulmonary Artery Thrombosis In Type 2 DM Patients Hospitalized With Covid-19
The American Journal of Medical Sciences and Pharmaceutical ResearchFor the first time on the Fergana Valley model, prognostic markers of the risk of thrombotic complications in COVID-19 patients with type 2 diabetes were studied. It was found that the level of glycemia, the concentration of proinflammatory cytokines IL-6, ferritin and CRP, and the marker of thrombus formation - d dimer, have a prognostic significance, with the maximum prognostic significance of the concentration of CRP. The prognostic significance of ultrasound in the aspect of thrombosis of the branches of the PA in patients with COVID-19 against the background of type 2 diabetes was established. Predictor markers are mean PA pressure, LV myocardial mass index, signs of increased intraventricular pressure in the RV, and evidence of peripheral venous thrombosis.
-
 Parameters of central hemodynamics in patients with ischemic heart disease, after revascularization
Parameters of central hemodynamics in patients with ischemic heart disease, after revascularization
Journal of Biomedicine and PracticePurpose of the study: to study the effect of the combination of valsartan and sacubitril on the indices of central hemodynamics in patients with coronary heart disease (CHD) within 2 years after revascularization. Material and research methods. The study included 320 patients with coronary artery disease who underwent coronary revascularization. All patients were divided into 2 groups: patients who received valsartan (group B, 160 people), patients who received ARNI - a combination of valsartan and sacubitrile molecules (group C, 160 people). At baseline and in dynamics after three months, at the end of the first and second years of follow-up after revascularization in patients with coronary artery disease systolic the blood pressure (SBP, mm Hg), diastolic blood pressure (DBP, mm Hg), heart rate in minute, the concentration of brain natriuretic peptide (BNP) in the blood were determined. Also, during echocardiography, the stroke volume of the heart, indexed to the body surface area (SI, ml / m2), the minute index (MI, ml / m2), the mean pressure in the pulmonary artery (PA, mm Hg) were determined. Research results. In the group of patients taking valsartan (group B), the relative dynamics of BNP concentration was -10.69 ± 0.55% by the 3rd month of observation, -21.24 ± 1.03% by the end of the 1st year, and -34, 39 ± 1.64% by the end of the 2nd year of observation. The inclusion of sacubitril in the therapy scheme contributed to a greater positive effect in reducing the BNP concentration: the relative dynamics of the BNP concentration was -10.30 ± 0.52% by the 3rd month of observation, - 21.91 ± 1.00% by the end of the first year of observation, and -39.28 ± 1.67% (p <0.05 significant difference with group B). By the end of the 1st and 2nd years of observation, the use of a combination of valsartan and sacubitril contributed to a more pronounced decrease in blood pressure (p <0.01), a more pronounced dynamics of MI (p <0.05) and a decrease in pressure in РA (significantly lower baseline indicators, p <0.05 and indicator in group B, p <0.01). Conclusion. The present study revealed a positive effect of revascularization and subsequent therapy of coronary artery disease with the inclusion of sacubitrile on the BNP concentration, blood pressure and mean pressure of pulmonary artery.
-
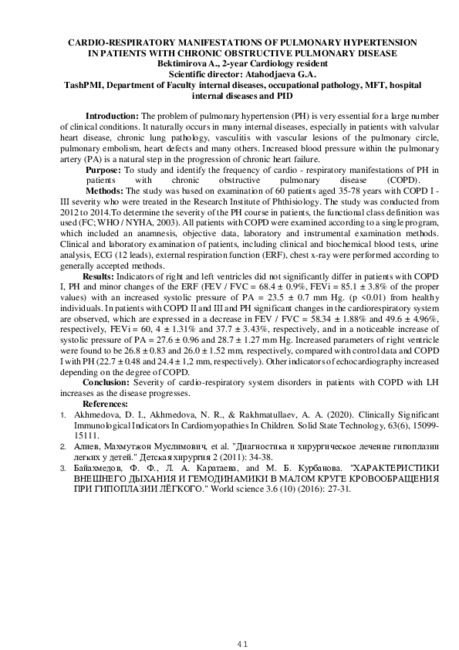 Cardio-respiratory manifestations of pulmonary hypertension in patients with chronic obstructive pulmonary disease
Cardio-respiratory manifestations of pulmonary hypertension in patients with chronic obstructive pulmonary disease
Scientific works of gifted youth and medicine of the XXI centuryThe problem of pulmonary hypertension (PH) is very essential for a large number of clinical conditions. It naturally occurs in many internal diseases, especially in patients with valvular heart disease, chronic lung pathology, vasculitis with vascular lesions of the pulmonary circle, pulmonary embolism, heart defects and many others. Increased blood pressure within the pulmonary artery (PA) is a natural step in the progression of chronic heart failure.
-
 Assessment of the possibility of improving functional reserves in patients With myocardial infarction and pulmonary comorbidity in the course of rehabilitationThe development of medical technologies and consequent aging of population requires multidisciplinary approaches in treating patients with myocardial infarction, as the number of comorbid pathologies usually increases with age. Comorbid pathology significantly complicates the process of diagnosis and treatment, results in patients disability, impedes adequate rehabilitation. The purpose of the given research was to analyze the relationship between pulmonary comorbidity and functional parameters of patients with myocardial infarction. 371 patients with acute myocardial infarction, who were undergoing inpatient stage of recovery, were examined. Entry criteria included: confirmed diagnosis of acute myocardial infarction and written informed consent of patients to participate in the study. Exit criteria included: psychiatric disorders, diseases of internal organs at the decompensation stage, as well as the presence of hemodynamically significant heart defects. The patients’ age was 66.16± 10.41 years. Of the patients participating in the research, 67.12% were male and 32.88% were female. Results and discussion. The development of myocardial infarction with underlying comorbid pulmonary pathology has its clinical and hemodynamic peculiarities, often complicated by left ventricular failure, and also has a tendency to the emergence of Dressier's syndrome, which aggravates the therapeutic process and limits the possibilities of rehabilitation. Limiting factors that significantly reduce the functionality of patients with myocardial infarction in combination with pulmonary pathology are smoking status, mitral and tricuspid valve regurgitation, elevated pulmonary artery pressure, as well as the Charlson Comorbidity Index. Smoking contributes to a significant deterioration of functional reserves in patients with myocardial infarction and pulmonary comorbidity, therefore, an indispensable part of the rehabilitation of these patients must be programs aimed at helping smokers to quit.
Assessment of the possibility of improving functional reserves in patients With myocardial infarction and pulmonary comorbidity in the course of rehabilitationThe development of medical technologies and consequent aging of population requires multidisciplinary approaches in treating patients with myocardial infarction, as the number of comorbid pathologies usually increases with age. Comorbid pathology significantly complicates the process of diagnosis and treatment, results in patients disability, impedes adequate rehabilitation. The purpose of the given research was to analyze the relationship between pulmonary comorbidity and functional parameters of patients with myocardial infarction. 371 patients with acute myocardial infarction, who were undergoing inpatient stage of recovery, were examined. Entry criteria included: confirmed diagnosis of acute myocardial infarction and written informed consent of patients to participate in the study. Exit criteria included: psychiatric disorders, diseases of internal organs at the decompensation stage, as well as the presence of hemodynamically significant heart defects. The patients’ age was 66.16± 10.41 years. Of the patients participating in the research, 67.12% were male and 32.88% were female. Results and discussion. The development of myocardial infarction with underlying comorbid pulmonary pathology has its clinical and hemodynamic peculiarities, often complicated by left ventricular failure, and also has a tendency to the emergence of Dressier's syndrome, which aggravates the therapeutic process and limits the possibilities of rehabilitation. Limiting factors that significantly reduce the functionality of patients with myocardial infarction in combination with pulmonary pathology are smoking status, mitral and tricuspid valve regurgitation, elevated pulmonary artery pressure, as well as the Charlson Comorbidity Index. Smoking contributes to a significant deterioration of functional reserves in patients with myocardial infarction and pulmonary comorbidity, therefore, an indispensable part of the rehabilitation of these patients must be programs aimed at helping smokers to quit.
Doctor's Herald -
 The state of central hemodynamics and endothelial function of peripheral vessels in patients with pulmonary hypertension
The state of central hemodynamics and endothelial function of peripheral vessels in patients with pulmonary hypertension
Scientific works of gifted youth and medicine of the XXI centuryChronic obstructive pulmonary disease (COPD) and severe bronchial asthma (BA) are some of the main causes of pulmonary arterial hypertension and account for more than 50% in the structure of pulmonary hypertension formation. The paper studies the state of central hemodynamics and endothelial function of peripheral vessels in patients with chronic obstructive pulmonary disease, bronchial asthma complicated by pulmonary hypertension (LH).
-
 Features of tuberculosis in children under COVID-19 pandemicThe aim of this study was to study the features of pulmonary TB in children who lived in family foci of TB infection and in foci of COVID-19 and TB. Materials and methods: The study was conducted in two groups of children formed according to the principle "case-control" study. The first group included 12 children with pulmonary tuberculosis from families where adults suffered with TB. The second group included 12 children with pulmonary tuberculosis from families where COVID-19 cases were initially registered, and then TB cases were registered. Indicators of the general blood test were analyzed. Results: Children with pulmonary TB who lived in family foci of TB infection and in foci of COVID-19 and TB did not differ in clinical forms of TB. On objective examination, vesicular respiration, single dry wheezing, systolic noise at the apex, and enlargement of peripheral lymph nodes were detected in children of both groups with almost the same frequency of occurrence. Children with pulmonary TB who lived in COVID-19 and TB family centers had peeling of the hands skin. This complaint was absent in children with pulmonary TB who lived in family foci of TB infection. When comparing the indicators of the general blood test, no significant differences were obtained. It was found that the ratio of monocytes to peripheral blood lymphocytes was higher in children with pulmonary TB who lived in COVID-19 and TB family foci, compared with children with pulmonary TB who lived in TB family foci. Conclusions: Further studies are needed to establish the prognostic value of the ratio of monocytes to peripheral blood lymphocytes in children with TB and COVID-19.
Features of tuberculosis in children under COVID-19 pandemicThe aim of this study was to study the features of pulmonary TB in children who lived in family foci of TB infection and in foci of COVID-19 and TB. Materials and methods: The study was conducted in two groups of children formed according to the principle "case-control" study. The first group included 12 children with pulmonary tuberculosis from families where adults suffered with TB. The second group included 12 children with pulmonary tuberculosis from families where COVID-19 cases were initially registered, and then TB cases were registered. Indicators of the general blood test were analyzed. Results: Children with pulmonary TB who lived in family foci of TB infection and in foci of COVID-19 and TB did not differ in clinical forms of TB. On objective examination, vesicular respiration, single dry wheezing, systolic noise at the apex, and enlargement of peripheral lymph nodes were detected in children of both groups with almost the same frequency of occurrence. Children with pulmonary TB who lived in COVID-19 and TB family centers had peeling of the hands skin. This complaint was absent in children with pulmonary TB who lived in family foci of TB infection. When comparing the indicators of the general blood test, no significant differences were obtained. It was found that the ratio of monocytes to peripheral blood lymphocytes was higher in children with pulmonary TB who lived in COVID-19 and TB family foci, compared with children with pulmonary TB who lived in TB family foci. Conclusions: Further studies are needed to establish the prognostic value of the ratio of monocytes to peripheral blood lymphocytes in children with TB and COVID-19.
Journal of hepato-gastroenterological research -
 Cavernous sinus thrombosis develops owing to purulent Infections of maxillofacial area and ENT-organs. Nowadays, It Is the complication at which mortality remains high (13-14 %), and according to some information reaches 50-70 %. In diagnostics of cavernous sinus thrombosis differential diagnostics of a cavernous sinus thrombosis with the general and eye pathologies Is Important. We have In detail considered exactly ophthalmologic symptoms that gives the copportunity to distinguish a thrombosis from a sepsis of not thrombotic character and by that influences on treatment and a disease outcome.
Cavernous sinus thrombosis develops owing to purulent Infections of maxillofacial area and ENT-organs. Nowadays, It Is the complication at which mortality remains high (13-14 %), and according to some information reaches 50-70 %. In diagnostics of cavernous sinus thrombosis differential diagnostics of a cavernous sinus thrombosis with the general and eye pathologies Is Important. We have In detail considered exactly ophthalmologic symptoms that gives the copportunity to distinguish a thrombosis from a sepsis of not thrombotic character and by that influences on treatment and a disease outcome. -
ETIOLOGY, PATHOGENESIS AND DIAGNOSIS OF ACUTE SENSORINEURAL HEARING LOSS WITH VASCULAR GENESIS
European International Journal of Multidisciplinary Research and Management StudiesAcute sensorineural hearing loss is an urgent condition that can develop irreversible and serious complications if is not treated on time. Hearing loss can develop suddenly or over several hours. Patients complain of congestion in the affected ear, noise in the ears, and often dizziness. Hearing loss is usually unilateral, and in 2% of cases it is bilateral. According to epidemiological data, the disease rate is 5-27 cases per 100,000 population. Unlike conductive tinnitus, sensorineural tinnitus is characterized by damage to the sound-receiving part of the unilateral auditory analyzer. The cranial artery is the only terminal artery that supplies the cranium with blood. A.auditivae is separated from the internal basilar artery in different situations. It separates from the lower anterior cerebral artery in 65% of cases, from the main one in 29%, and from the lower posterior cerebral artery in 6% of cases.
-
EPIDEMIOLOGICAL AND CYTO-MORPHOLOGICAL SPECTRUM OF PULMONARY LESION BY CT GUIDED FNAC
The American Journal of Medical Sciences and Pharmaceutical ResearchBackground: CT-guided fine-needle aspiration cytology is an established, indeed effective and precise method for diagnosing of pulmonary lesions. Though this procedure has the possibility to lead lung complications. Therefore, this study aimed to learn about the pathological spectrum of pulmonary lesions, examine the pattern of FNAC diagnosis of lung lesions, and analyse and compare the data with published figures.
Material & method: This study was carried out at the Pathology Department of Tairunnessa Memorial Medical College and Hospital, as well as the Popular Diagnostic Center in Gazipur, Bangladesh, where all cases were FNAC and cytologically diagnosed. From September 2000 to April 2022, a total of 171 cases were evaluated. All of the patients had nodular or mass lesions in their lungs and were diagnosed with a CT-guided FNAC by following a standard procedure.
Result: Out of 171 cases about 119 (69.59%) were male and 52 (30.40 %) female. It was noticed that approximately 117 (68.42%) were malignant cases. Of these, most common malignancy was adenocarcinoma (43.27%). There were about 31.67 % benign lung lesions cases. Among them, 17.54%, 8.87%, 3.5%, and 1.67% cases had pulmonary inflammatory lesions, tuberculosis, aspergillosis and abscess, respectively.
Conclusion: CT guided FNAC can diagnose pulmonary lesion fairly and accurately as well as may leading to less morbidity & mortality as treatment can be started early.
-
 ANTAGONISTS OF ENDOTHELIN RECEPTORS IN THE PATHOGENETIC TREATMENT OF PULMONARY ARTERIAL HYPERTENSION (REVIEW)Theoretical aspects of the using of endothelin receptor antagonists in the pathogenetic treatment of pulmonary hypertension are investigated. A comparative analysis of selective and non-selective endothelin receptor antagonists in the treatment of pulmonary arterial hypertension is performed. Special attention is paid to the role of endothelin in the pathogenesis of pulmonary hypertension. The pharmacodynamic and pharmacokinetic features of individual representatives of endothelin receptor antagonists, such as bosentan, ambrisentan and macitentan, the effect of these drugs on clinical symptoms, hemodynamic parameters, and load tolerance were studied.
ANTAGONISTS OF ENDOTHELIN RECEPTORS IN THE PATHOGENETIC TREATMENT OF PULMONARY ARTERIAL HYPERTENSION (REVIEW)Theoretical aspects of the using of endothelin receptor antagonists in the pathogenetic treatment of pulmonary hypertension are investigated. A comparative analysis of selective and non-selective endothelin receptor antagonists in the treatment of pulmonary arterial hypertension is performed. Special attention is paid to the role of endothelin in the pathogenesis of pulmonary hypertension. The pharmacodynamic and pharmacokinetic features of individual representatives of endothelin receptor antagonists, such as bosentan, ambrisentan and macitentan, the effect of these drugs on clinical symptoms, hemodynamic parameters, and load tolerance were studied.
Journal of Cardiorespiratory Research -
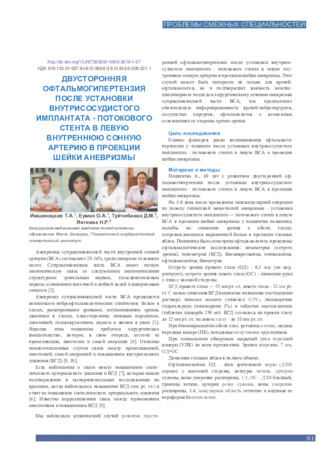 Bilateral ophthalmohypertension after the installation of an intravascular implant - a flow stent in the left internal carotid artery in the projection of the neck of the aneurysm
Bilateral ophthalmohypertension after the installation of an intravascular implant - a flow stent in the left internal carotid artery in the projection of the neck of the aneurysm
in Libraryassessment of risk factors for the occurrence of ophthalmohypertension in a patient after the installation of an intravascular implant - a flow stent in the left internal carotid artery (ICA) in the projection of the aneurysm neck. Material and Methods: Patient A., 69 years old, with the development of bilateral ophthalmohypertension after the installation of an intravascular implant - a flow stent in the left ICA in the projection of the aneurysm neck. Results: Based on the examination of the patient and the study of all possible risk factors for the occurrence of ophthalmohypertension, confirmed by the data of modern literature, we can assume a multifactorial cause of bilateral ophthalmohypertension after the installation of an intravascular implant - a flow stent in the left internal carotid artery in the projection of the aneurysm neck. Conclusions: An interdisciplinary approach to the surgical treatment of an aneurysm of the supracune-shaped part of the internal carotid artery is important.
-
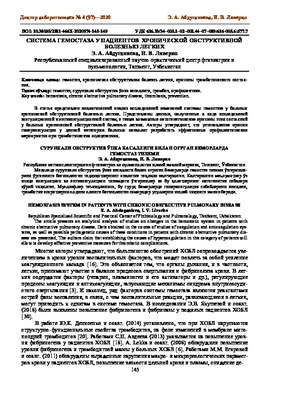 Republican Specialized Scientific and Practical Center of Phthisiology and Pulmonology, Tashkent, Uzbekistan The article presents an analytical analysis of studies on changes in the hemostatic system in patients with chronic obstructive pulmonary disease. Data obtained in the course of studies of coagulation and anticoagulation systems, as well as possible pathogenetic causes of these conditions in patients with chronic obstructive pulmonary disease are presented. The authors claim that establishing the causes of hypercoagulation in this category of patients will allowr to develop effective preventive measures for thrombotic complications.
Republican Specialized Scientific and Practical Center of Phthisiology and Pulmonology, Tashkent, Uzbekistan The article presents an analytical analysis of studies on changes in the hemostatic system in patients with chronic obstructive pulmonary disease. Data obtained in the course of studies of coagulation and anticoagulation systems, as well as possible pathogenetic causes of these conditions in patients with chronic obstructive pulmonary disease are presented. The authors claim that establishing the causes of hypercoagulation in this category of patients will allowr to develop effective preventive measures for thrombotic complications. -
Predictors Of The Development Of Chronic Kidney Disease In Patients With Chronic Obstructive Pulmonary Disease
The American Journal of Medical Sciences and Pharmaceutical ResearchThe aim of the study was to identify predictors of decreased glomerular filtration in patients with chronic obstructive pulmonary disease (COPD). Materials and methods. We analyzed 145 case histories of patients diagnosed with COPD. The majority (84.1%, n = 122) of them are males (the average age of men is 60.7 ± 0.9 years, the average age of women is 62.0 ± 2.7 years). A comparative analysis of the prevalence of risk factors for chronic kidney disease (CKD) in patients with COPD: age, gender, smoking, arterial hypertension, overweight, etc. The glomerular filtration rate (GFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD – EPI) formula, according to which the patients were divided into 6 groups: group 1 - hyperfiltration, group 2 - GFR CKD – EPI ≥ 90 ml / min / 1 , 73 m2, 3rd - GFR CKD – EPI 60–89 ml / min / 1.73 m2, 4th - GFR CKD – EPI 45–59 ml / min / 1.73 m2, 5th - GFR CKD – EPI 30 - 44 ml / min / 1.73 m2 and 6th-GFR CKD-EPI <30 ml / min / 1.73 m2. Results. Patients with COPD have a high incidence of CKD risk factors. A correlation was found between the prevalence of CKD risk factors and the severity of COPD. The main predictors of the development of CKD in patients with COPD: duration of COPD> 9 years, body mass index> 26.5 kg / m2, smoking index> 51.3, albumin> 44.0 g / l, total protein> 70.0 g / L, forced expiratory volume in the first second ≤ 1.6 L, right atrial size> 35.5 mm, systolic pressure in the pulmonary artery> 36.6 mm Hg. Art., the thickness of the posterior wall of the left ventricle> 10.5 mm, Tiffno's index ≤ 62%. Conclusion. It was found that patients with COPD
-
 PRINCIPLES OF PROVIDING DENTAL CARE TO PATIENTS WITH PULMONARY TUBERCULOSISThe presence of odontogenic lesions in patients with pulmonary tuberculosis is characterized by specific symptoms of intoxication, changes in blood, destruction of the lungs, changes in immunoglobulins and immune components. The aim of the study was to improve the effectiveness of prevention and treatment of dental caries in patients with tuberculosis. Dental care in the treatment of patients with pulmonary tuberculosis has its own characteristics, which depend on the course of the disease, the degree of spread. It has been established that patients undergoing treatment at an anti-tuberculosis dispensary should receive not only chemotherapy, but also dental care after a dental examination. Treating physicians should work with dentists to treat the entire body of a pulmonary tuberculosis patient.
PRINCIPLES OF PROVIDING DENTAL CARE TO PATIENTS WITH PULMONARY TUBERCULOSISThe presence of odontogenic lesions in patients with pulmonary tuberculosis is characterized by specific symptoms of intoxication, changes in blood, destruction of the lungs, changes in immunoglobulins and immune components. The aim of the study was to improve the effectiveness of prevention and treatment of dental caries in patients with tuberculosis. Dental care in the treatment of patients with pulmonary tuberculosis has its own characteristics, which depend on the course of the disease, the degree of spread. It has been established that patients undergoing treatment at an anti-tuberculosis dispensary should receive not only chemotherapy, but also dental care after a dental examination. Treating physicians should work with dentists to treat the entire body of a pulmonary tuberculosis patient.
Journal of oral medicine and craniofacial research -
Pulmonary Echinococcosis Surgery
The American Journal of Medical Sciences and Pharmaceutical ResearchWe present an analysis of the results of surgical treatment of 182 patients with pulmonary echinococcosis (126 patients with uncomplicated and 56 with complicated pulmonary echinococcosis). Of these, only in 23 patients out of 25 planned, it was possible to carry out echinococcectomy purely thoracoscopically through trocar punctures. In 134 cases, videothoracoscopic echinococectomy was performed using a mini-access. In case of bilateral localization of cysts, stage-by-stage operations were performed in 7 patients, and in 3 (36.36%) cases - single-stage echinococcectomy. Echinococcectomy from the lung was performed in 25 patients using a wide thoracotomy approach. In 134 cases, videothoracoscopic echinococectomy was performed using a mini-access. In case of bilateral localization of cysts, stage-by-stage operations were performed in 7 patients, and in 3 (36.36%) cases - single-stage echinococcectomy. Echinococcectomy from the lung was performed in 25 patients using a wide thoracotomy approach. All patients underwent anterolateral thoracotomy. Basically (97.67%) performed organ-preserving operations with the elimination of the residual cavity in the light suture plastics in various modifications. In 2 patients with marginal location and pneumocirrhosis, marginal resection of the lung with an echinococcal cyst was performed.With combined echinococcosis of the lungs and liver, 10 patients were operated on. 6 patients underwent surgical interventions on the lungs and liver through separate approaches at the same time. The use of minimally invasive techniques for pulmonary echinococcosis is possible in more than 2/3 of patients.
-
 Predictors of risk of progression of pulmonary parenchymal fibrosis and unfavorable endpoints in patients with postcovid syndrome
Predictors of risk of progression of pulmonary parenchymal fibrosis and unfavorable endpoints in patients with postcovid syndrome
Journal of Biomedicine and PracticePurpose of the study. Based on a retrospective analysis, to determine prognostic markers for the progression of fibrosis of the pulmonary parenchyma and the development of unfavorable endpoints in patients with postcovid syndrome.
Material and research methods. The material of the study was the case histories of 128 patients who underwent COVID-19 and are in early medical rehabilitation. A retrospective analysis of the data of case histories and their statistical processing were carried out.
Research results. Patients with progressive pulmonary fibrosis were more comorbid (p<0.001). BA (p <0.05), CIPD (p <0.05), obesity and steatohepatitis (p <0.001) and thromboembolic events within a month after discharge from the infectious hospital (p <0.001) were significantly more frequent in them. Thromboembolic events occurred in 66 patients (51.56%), 12 patients died (9.38%), the combined endpoint (death + thromboembolism) occurred in 70 patients (54.69%). The risk of adverse endpoints is significantly higher in patients with severe and extremely severe COVID-19. In these patients, the average number of background pathologies was significantly higher (p <0.001), among which COPD (p <0.001), type 2 diabetes (p <0.05), obesity and steatohepatitis (p <0.001), Parkinson's syndrome ( p <0.05). Also, the group of patients with the development of thromboembolism and deaths was distinguished by more pronounced lung damage (p <0.05), a higher incidence of severe and extremely severe infections (chi square = 6.98, p <0.01).
Conclusion. Retrospective analysis showed that the risk of progression of fibrosis of the pulmonary parenchyma in patients with COVID-19 increases in the presence of AD by 1.83 times (p<0.05), CIBD - 2.46 times (p <0.05), obesity and steatohepatitis - 7.22 times (p <0.001), the development of thromboembolic events during the first month - 9.39 times (p <0.001). The risk of developing a combined unfavorable endpoint (death and thromboembolic events) COVID-19 increases 1.63 times in severe and extremely severe disease, 2.33 times in the presence of COPD (p <0.001), 1.63 times - in the presence of type 2 diabetes (p <0.05), 3.64 times - in the presence of obesity and steatohepatitis (p <0.001). -
 Effectiveness of intravitreal administration of the kenalog in central venous retinal vein thrombosisUnder our supervision there were 12 patients with thrombosis of Central vein of retina treated in the 1st clinic of SamMI the eye Department. The age of patients ranged from 45 to 69 years, the average was 52.6 years. Of them women to 7 men – 5. The cause of retinal vein thrombosis were mainly hypertension and diabe- tes, or a combination. The effectiveness of intravitreal injection of kenalog is probably connected with the in- crease in the concentration of steroids in the lesion, leading to the decrease in retinal edema and restoration of elements of the retina due to the longer effect of the drug
Effectiveness of intravitreal administration of the kenalog in central venous retinal vein thrombosisUnder our supervision there were 12 patients with thrombosis of Central vein of retina treated in the 1st clinic of SamMI the eye Department. The age of patients ranged from 45 to 69 years, the average was 52.6 years. Of them women to 7 men – 5. The cause of retinal vein thrombosis were mainly hypertension and diabe- tes, or a combination. The effectiveness of intravitreal injection of kenalog is probably connected with the in- crease in the concentration of steroids in the lesion, leading to the decrease in retinal edema and restoration of elements of the retina due to the longer effect of the drug
Journal problems of biology and medicine -
Замонавий тиббиёт радиацион тасвирлаш усулларининг сезиларли даражада ривожланиши ва дсярли барча анатомии сохаларни бахолаш учуй мослаштириши мумкин булган турли режимларнинг пайдо булиши билан ажралиб туради. Ушбу тадкикот натижаларига кура, COV1D-19 билан боглик булган кавсрноз синус тромбозини эрта аниклаш учун тасвирлаш методологиясини таклиф килади. Тромбнинг борлигини аниклаш имкон бсрадиган махсус рсжимларда МРТ тасвирларини тавсифлаш ва изохлаш амалга оширилди. Тадкикот шуни курсатдики, тавсия этилган тасвирлаш усули узига хос аломатлар пайдо булишидан олдин бсморларда тромбозни эрта аниклашга имкон бсради.
-
There were examined 57 eyes with thrombosis of central retinal vein and its branches. The course of treatment with activated autoplasm lasted 10-12 days as parabulbar injection in the close of 0.5 ml in the affected eye and intramuscular injection — 3.0-5.0 ml daily. The results showed that activated autoplasm in the course of conservative therapy of retinal vein thrombosis had a positive influence on clinical function state of the affected eye.
-
 Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Catalog of abstractsRelevance of the problem.Despite the great successes of angiosurgery, the problem of surgical treatment of abdominal aortic aneurysms does not lose its relevance. World health statistics records a steady increase in the incidence of abdominal aortic aneurysm (ABA). According to L.J. Melton et al. (1984) and L.K. Bickerstaff et al. (1984) in the USA the number of patients with abdominal aortic aneurysm has increased 7 times in 30 years since 1951. In England and Wales, according to F.G. Fowkers et al. (1989) for the same period revealed a 20-fold increase in abdominal aortic aneurysms in men and 11-fold in women. According to the results of multicentre screening studies ABA was detected in 8% of the examined (E.S. Vourvouri, 2001), and in the age group of 64-69 years ABA was detected in 5.7% of the examined, and in the age group of 75-81 years - in 8.9% (R.A.P. Skott et al., 2001). A similar trend is observed in other countries. Accordingly, mortality from ABA is also increasing - aneurysm rupture in a number of countries is one of the ten most frequent causes of death among elderly and senile people (F.A. Lederle et al., 1990)
Currently, planned aneurysm resection has become a recognised standard of radical treatment of ABA patients and the number of these operations is steadily increasing. For example, about 40,000 ABA resections are performed annually in the USA (J.J. Grange et al., 1997). In Sweden during the period from 1987-89 to 1993-95 the number of ABA operations increased 5 times and currently 10 operations per 100,000 population are performed (A.Hallin et al., 2001), although this is 1.5 - 2 times less than the required number. However, postoperative lethality is still quite high and makes 5-7% (A.V.Pokrovskiy et al., 1992; Y.V.Belov et al., 1992; V.V.Vakhidov et al., 1992; A.W. Bradbury et al. Bradbury et al., 1997; A.Hallin et al., 2001).
E.W. Steyeberg et al. (1995) summarised the data of literature on 17238 ABA resection operations and gave an average mortality of 6.8%.
Multicentre studies in five major hospitals in the Netherlands found that only 74% of patients underwent ABA resection without complications; 26% had some complications, 9% of which were severe and 4.1% of which were fatal (G.J. Akkersdijk et al., 1998). Similar results were obtained in the Canadian Cooperative Study (K.W. Johnston et al., 1990). It was established that the peculiarity of complications in the majority of patients was their systemic character (L.L. Lau et al, 2001) The course of the postoperative period is most often complicated by cardiac, respiratory, renal, cerebrovascular, as well as complications associated with thrombosis and bleeding (W.E. Lloyd et al., 1996; R.D. Sayers et al., 1997; J.D. Blankenstein et al., 1998; R. Ayari et al., 1998). Ayari et al., 2001)
The undisputed leadership, without doubt, belongs to cardiac complications, the incidence of which varies from 10% to 20%. Moreover, cardiac complications account for 50-70% of total mortality. Cerebrovascular complications, although not uncommon, account for no more than 1-1.5%, but their mortality reaches 40%. Complications associated with thromboses and haemorrhages in the perioperative period reach 2-5% (M.M.Reigel et al., 1987; K.W.Johnson et al., 1990; N.Franklin et al., 1993; A.A.Milne et al., 1994).
Certainly, a large number of complications after resection of abdominal aortic aneurysms is caused by the initial severity of patients' condition, however, many unresolved tactical and technical issues of patients' preparation for the operation, stage of performance in case of combined lesions of several vascular basins play a practically significant role. Adequate management of the operation itself and the immediate postoperative period is no less important, taking into account the possibility of such dreadful complications as thrombosis and embolism, cerebral and cardiac death. Until now there is no unified complex analysis of the results of treatment of uncomplicated abdominal aortic aneurysms and, accordingly, recommendations for the prevention of possible complications.
All this determined our aim and objectives of the study.
The aim of the study is to improve the results of surgical treatment of ABA by developing an effective system for determining the main risk factors of surgical treatment and optimal surgical tactics to prevent possible complications.
Scientific novelty.For the first time a complex analysis of indications and contraindications to surgical treatment of abdominal aortic aneurysms was carried out
The most significant concomitant pathology capable to lead to formidable complications and lethality during the intervention and in the nearest postoperative period was revealed. Adequate measures of their prevention and treatment were proposed.
The algorithm of surgical treatment tactics for patients with combined pathology of coronary arteries and aortic arch branch lesions was developed
The state of haemostasis system at all stages of reconstructive surgery on abdominal aorta, starting from skin incision to wound closure, was studied for the first time.
Conclusions:
1. The proposed original classification of ABA, based on mutual dependence on the etiology of the disease, localisation, concomitant diseases, clinic and its course, allows to determine the strategy of early diagnosis, to estimate the most significant risk factors, the stage of intervention in combined lesions of adjacent and distant vascular basins and, ultimately, to determine the ways to reduce complications and mortality in patients with ABA.
2. The most informative methods of ABA diagnostics are duplex scanning and computed tomography. Non-invasive diagnostics capabilities are enough to determine the aneurysm size, its relation to the renal arteries, as well as to find out the state of visceral branches and aortic bifurcation. Abdominal aortography is indicated in patients with concomitant arterial hypertension to identify the state of the renal arteries.
3. Significant risk factors in these patients are ischaemic heart disease (44.1%), arterial hypertension (49%), haemostasis disorders (almost 100%).
4. The leading concomitant disease in the development of postoperative complications is ischaemic heart disease. Its share in abdominal aortic aneurysms is 40%. Postoperative cardiac complications reach 14.9%. Diagnostics of ischaemic heart disease should be based on the stage-by-stage detection of coronary lesions and its functional-compensatory abilities.
5. The main complications of the postoperative period after ABA resections are acute heart failure (14,9%), cerebral circulatory disorders (1,5%), acute renal failure (3,33%).
6. When significant coronary vascular channel lesions are detected in patients with ABA, it is fundamental to solve the issue of intervention staging. At 3-4 functional classes of circulatory insufficiency, appearance of new zones of hypo- or akinesia, decrease of ejection fraction below 40%, the first stage should be myocardial revascularisation surgery
7. In patients with combined lesions of brachiocephalic vessels in patients with ABA it is reasonable to assess the cerebral blood flow. In the presence of 70% or more stenosis of VCA, presence of embologenic plaque, bilateral haemodynamically significant stenosis it is necessary to perform carotid artery intervention as the first stage.
8. One of the most difficult problems of reconstructive operations in ABA is the contiguous lesion of renal and visceral branches of the abdominal aorta. The principle is their one-stage reconstruction. The types of reconstruction of these branches should be variable depending on the volume and extent of the pathological process.
9. Patients with aneurysmal lesion of abdominal aorta initially always have significant disorders of haemostasis system. In 30% of patients with occlusive diseases of aorta and its branches in the preoperative period the activity of thrombocytic-vascular link of hemostasis is increased, antithrombotic ability of vascular wall endothelium is decreased and blood rheological properties are disturbed. Activation of fibrinolysis was noted in patients with aneurysmal lesion of abdominal aorta.
10. During the operation for abdominal aortic aneurysmal lesion, after starting the blood flow the level of plasminogen increases additionally by 30%, which is a risk factor for haemorrhagic complications in the perioperative period. On the 1-3 day after the operation there is a significant decrease of blood anticoagulant potential - antithrombin-Sh by 25-27%, protein C by 23-25%. This period is the most dangerous in terms of thrombohemorrhagic complications development.
11. When using standard heparin during the operation there is a consumption of antithrombin-Sh by 30-45% and increase of platelet aggregation by 10%, which is a threatening condition for the occurrence of thrombosis of deep veins of the lower extremities with subsequent TELA. When using fraxiparin during reconstructive vascular surgeries the consumption of antithrombin-Sh and increase in platelet aggregation do not occur, prothrombin time, activated partial thromboplastin time, thrombin time are lengthened insignificantly that testifies to expediency of its use for prevention of thrombohemorrhagic complications.
12. Application of the diagnostic methods proposed by us to detect the main risk factors during the operation and in the nearest postoperative period, use of the algorithm of stage and volume of intervention allowed to reduce significantly the number of threatening complications, thus the lethality decreased 4 times, and the number of non-fatal complications - 4 times non-fatal complications - 1.5 times. -
 BILATERAL OPHTHALMOHYPERTENSION AFTER INSTALLATION OF AN INTRAVASCULAR IMPLANT – FLOW STENT INTO THE LEFT INTERNAL CAROTID ARTERY IN THE PROJECTION OF THE NECK OF THE ANEURYSMA clinical case of the development of bilateral ophthalmic hypertension after the installation of an intravascular implant - a flow stent in the left internal carotid artery in the projection of the aneurysm neck is described, which may be of interest not only to ophthalmologists, but also confirms the importance of an interdisciplinary approach in the surgical treatment of supraclinical aneuiysm (internal carotid artery aneurysm), which implies die mandatory awareness of neurosurgeons, vascular surgeons, ophthalmologists about possible sensations from tire organ of vision.
BILATERAL OPHTHALMOHYPERTENSION AFTER INSTALLATION OF AN INTRAVASCULAR IMPLANT – FLOW STENT INTO THE LEFT INTERNAL CAROTID ARTERY IN THE PROJECTION OF THE NECK OF THE ANEURYSMA clinical case of the development of bilateral ophthalmic hypertension after the installation of an intravascular implant - a flow stent in the left internal carotid artery in the projection of the aneurysm neck is described, which may be of interest not only to ophthalmologists, but also confirms the importance of an interdisciplinary approach in the surgical treatment of supraclinical aneuiysm (internal carotid artery aneurysm), which implies die mandatory awareness of neurosurgeons, vascular surgeons, ophthalmologists about possible sensations from tire organ of vision.
Stomatologiya -
 Study of the development level of risk factors in dangerous tumors causing lonely arterial thromboembolia
Study of the development level of risk factors in dangerous tumors causing lonely arterial thromboembolia
in LibraryOur study showed that VTE is one of the most serious complications in patients with oncopathology and determines the course of the disease, requires dynamic monitoring of hemodynamic parameters and timely administration of both pharmacological and mechanical means of preventing thrombosis. Preventing the development of VTE is one of the important steps to increase the survival of cancer patients
-
 POLYMORPHISMS ARG506GLN OF THE F5 GENE, G20210A OF THE F2 GENE, GLU429ALA OF THE MTHFR GENE, ASP919GLY OF THE MTR GENE OF THROMBOPHILIA GENES - AS PREDICTORS OF THROMBOTIC COMPLICATIONS IN PATIENTS WITH CHRONICAL OBSTRUCTIVE PULMONARY DISEASEThe study analyzed the results of studies of the genes of the most common thrombophilia in patients with chronic obstructive pulmonary disease in the Uzbek population. As a result, the authors discovered genetic predictors of thrombotic complications by polymorphism of Arg506Gln genes of the F5 gene; polymorphism G20210A of the F2 gene; polymorphism Glu429Ala of the MTHFR gene, among which a significant predominance of mutant alleles, mutant genotypes, and a predisposing heterozygous form of the genotype of polymorphisms 20210 G / A of the F2 gene, Arg506Glu of the F5 gene, 1298 A> C of the MTHFR gene was found. The authors also noted that, in patients with COPD in the Uzbek population, no associations of the Asp919Gly polymorphism of the MTR gene were found.
POLYMORPHISMS ARG506GLN OF THE F5 GENE, G20210A OF THE F2 GENE, GLU429ALA OF THE MTHFR GENE, ASP919GLY OF THE MTR GENE OF THROMBOPHILIA GENES - AS PREDICTORS OF THROMBOTIC COMPLICATIONS IN PATIENTS WITH CHRONICAL OBSTRUCTIVE PULMONARY DISEASEThe study analyzed the results of studies of the genes of the most common thrombophilia in patients with chronic obstructive pulmonary disease in the Uzbek population. As a result, the authors discovered genetic predictors of thrombotic complications by polymorphism of Arg506Gln genes of the F5 gene; polymorphism G20210A of the F2 gene; polymorphism Glu429Ala of the MTHFR gene, among which a significant predominance of mutant alleles, mutant genotypes, and a predisposing heterozygous form of the genotype of polymorphisms 20210 G / A of the F2 gene, Arg506Glu of the F5 gene, 1298 A> C of the MTHFR gene was found. The authors also noted that, in patients with COPD in the Uzbek population, no associations of the Asp919Gly polymorphism of the MTR gene were found.
Journal of Cardiorespiratory Research -
 The effect of pulmonary tuberculosis on the mental state of adolescentsA comparative assessment of the psychological characteristics of adolescents with pulmonary tuberculosis. The personal characteristics of 100 adolescents aged 13-17 treated at the Samarkand Regional Center for Tuberculosis and Pulmonology, as well as various features of newly diagnosed respiratory tuberculosis, were studied, including 58 (58%) girls and 42 (42%) boys. Patients with MDR-TB see themselves as altruistic, more likely to feel willing to sacrifice their own interests, help others, and show compassion. Such adolescents tend to make a pleasant impression on others and idealize interpersonal relationships that typically show tenderness, sensitivity, and compassion for them (p <0.05). In adolescents with pulmonary tuberculosis with widespread processes, personality traits that determine the formation of neurosis were observed: insecurity, emotional instability, anxiety, weakness. In a small group with limited lesions, high rates of resentment and hostility were rare.
The effect of pulmonary tuberculosis on the mental state of adolescentsA comparative assessment of the psychological characteristics of adolescents with pulmonary tuberculosis. The personal characteristics of 100 adolescents aged 13-17 treated at the Samarkand Regional Center for Tuberculosis and Pulmonology, as well as various features of newly diagnosed respiratory tuberculosis, were studied, including 58 (58%) girls and 42 (42%) boys. Patients with MDR-TB see themselves as altruistic, more likely to feel willing to sacrifice their own interests, help others, and show compassion. Such adolescents tend to make a pleasant impression on others and idealize interpersonal relationships that typically show tenderness, sensitivity, and compassion for them (p <0.05). In adolescents with pulmonary tuberculosis with widespread processes, personality traits that determine the formation of neurosis were observed: insecurity, emotional instability, anxiety, weakness. In a small group with limited lesions, high rates of resentment and hostility were rare.
Journal of hepato-gastroenterological research