Library search
Search Results
-
Features Of The Clinical And Laboratory Course Of Tuberculosis Lymphadenopathy In Patients Without And With HIV Infection
The American Journal of Medical Sciences and Pharmaceutical ResearchTuberculous lymphadenopathy without HIV infection, in comparison with those with HIV infection, was characterized by a more favorable clinical course, limited lesion and, especially important, limited caseous-necrotic changes. Analysis of the histological picture of the removed lymph nodes in patients with HIV-i made it possible to distinguish three activities of tuberculous lymphadenopathy: an inactive phase (with a predominance of a productive cellular reaction) - in 3 patients (5.3%), an active (with a predominantly productive-necrotic tissue reaction) - in 11 patients (19.3%), the phase of progression of the pathological process (mainly necrotic lesions, suppuration and formation of fistulas) - in 43 patients (75.4%). It was found that the inactive phase is 5.5 times more common in patients without HIV than in patients with HIV (29.3% and 5.3%, respectively, P˂0.001), while the active phase and the progression phase was 1.5 and 1.3 times more frequent in patients with HIV than in patients without HIV (19.3% and 13.1, respectively, P˃0.5; 75.4% and 57, 6%, respectively, P˂0.02).
-
 RISK FACTORS AND LIFE`S QUALITY CONDITION OF CHILDREN WITH LATENT TUBERCULOUS INFECTIONBackground. Latent tuberculosis infection is an asymptomatic condition in which patients carry the bacteria, but do not show any sign of illness, however they are at risk of disease activation at any time in the future. Latent tuberculosis infection is often not to affect the quality of life of patients. Preventive treatment of latent tuberculosis infection can reduce the risk of activation; however, this treatment can produce such side effects as well as psychosocial challenges, which can increase stigma and psychological stress. These factors can impair the Quality of Life of patients in term of physical, mental and social well-being. Understanding of influence of latent tuberculosis infection on the physical and mental well-being of these patients is important as successful strategies to reduce the tuberculosis burden globally. Our purpose is to explore patients during diagnosis and treatment of latent tuberculosis infection, measure their quality of life. Objective. During 2019-2020 were examined 100 children 0-14 yearsold. Methods. Quality of life was defined with the help of questionnaire PedsQL version 4.0 (the Russian version), for children. Results. at children with active tuberculosis specific process has a most negative influence upon quality of life, comparatively temporary negative influence has latent tuberculous infection. Conclusions. With provision of latency currents of infecting with mycobacteria of tuberculosis, indicators of quality of life should be considered as one of defining, reflecting psychological component adaptation of child, and can be recommended to enter in program of examination and dispensary observation of children with latent tuberculous infection.
RISK FACTORS AND LIFE`S QUALITY CONDITION OF CHILDREN WITH LATENT TUBERCULOUS INFECTIONBackground. Latent tuberculosis infection is an asymptomatic condition in which patients carry the bacteria, but do not show any sign of illness, however they are at risk of disease activation at any time in the future. Latent tuberculosis infection is often not to affect the quality of life of patients. Preventive treatment of latent tuberculosis infection can reduce the risk of activation; however, this treatment can produce such side effects as well as psychosocial challenges, which can increase stigma and psychological stress. These factors can impair the Quality of Life of patients in term of physical, mental and social well-being. Understanding of influence of latent tuberculosis infection on the physical and mental well-being of these patients is important as successful strategies to reduce the tuberculosis burden globally. Our purpose is to explore patients during diagnosis and treatment of latent tuberculosis infection, measure their quality of life. Objective. During 2019-2020 were examined 100 children 0-14 yearsold. Methods. Quality of life was defined with the help of questionnaire PedsQL version 4.0 (the Russian version), for children. Results. at children with active tuberculosis specific process has a most negative influence upon quality of life, comparatively temporary negative influence has latent tuberculous infection. Conclusions. With provision of latency currents of infecting with mycobacteria of tuberculosis, indicators of quality of life should be considered as one of defining, reflecting psychological component adaptation of child, and can be recommended to enter in program of examination and dispensary observation of children with latent tuberculous infection.
Journal of Cardiorespiratory Research -
 TO THE QUESTION OF THE COURSE OF PULMONARY TUBERCULOSIS WITH DISEASES OF THE CARDIOVASCULAR SYSTEMWith pulmonary tuberculosis, even in the early stages of the development of a specific process, changes in the cardiovascular system are noted. The high sensitivity of the vascular system to tuberculous intoxication has long been established. With the combination of active tuberculosis process with cardiovascular pathologies, great difficulties arise in connection with the need for a comprehensive antibacterial therapy for tuberculosis and the simultaneous treatment of concomitant diseases, including vascular pathology. The purpose of this article is to study the features of the course of cardiovascular lesions in patients with pulmonary tuberculosis during various periods of the disease. Of particular interest is the study of changes in the right and left parts of the heart in those cases when signs of hypertension are not detected on the basis of clinical, radiological and electrocardiographic studies. With the combination of active tuberculous process with cardiovascular pathology, great difficulties arise in connection with the need for complex antibacterial therapy for tuberculosis and the simultaneous treatment of concomitant diseases, including vascular pathology.
TO THE QUESTION OF THE COURSE OF PULMONARY TUBERCULOSIS WITH DISEASES OF THE CARDIOVASCULAR SYSTEMWith pulmonary tuberculosis, even in the early stages of the development of a specific process, changes in the cardiovascular system are noted. The high sensitivity of the vascular system to tuberculous intoxication has long been established. With the combination of active tuberculosis process with cardiovascular pathologies, great difficulties arise in connection with the need for a comprehensive antibacterial therapy for tuberculosis and the simultaneous treatment of concomitant diseases, including vascular pathology. The purpose of this article is to study the features of the course of cardiovascular lesions in patients with pulmonary tuberculosis during various periods of the disease. Of particular interest is the study of changes in the right and left parts of the heart in those cases when signs of hypertension are not detected on the basis of clinical, radiological and electrocardiographic studies. With the combination of active tuberculous process with cardiovascular pathology, great difficulties arise in connection with the need for complex antibacterial therapy for tuberculosis and the simultaneous treatment of concomitant diseases, including vascular pathology.
Journal of Cardiorespiratory Research -
 A clinical case of a rare tuberculous lesion of the RIBThe rarest localization of tuberculosis of flat bones is the ribs and sternum. The specific lesion of the ribs is caused by the close contact of the chest organs: the lymphatic and circulatory systems of the pleura, lungs, and heart. In the literature data, cases of the middle ribs damage, mainly the anterior surface, arc given. The erasure of clinical symptoms and reduced alertness towards tuberculosis, leads to a complicated course of a specific lesion.
A clinical case of a rare tuberculous lesion of the RIBThe rarest localization of tuberculosis of flat bones is the ribs and sternum. The specific lesion of the ribs is caused by the close contact of the chest organs: the lymphatic and circulatory systems of the pleura, lungs, and heart. In the literature data, cases of the middle ribs damage, mainly the anterior surface, arc given. The erasure of clinical symptoms and reduced alertness towards tuberculosis, leads to a complicated course of a specific lesion.
Инновационные подходы к диагностике, лечению и профилактике туберкулеза и неспецефической респираторной патологии у взрослых и детей -
 Informativity of magnetic-resonance tomography in diagnosis of tuberculosis spondilites and its complications89 magnetic resonance tomograms, which were performed by 72 patients with TS, were analyzed. A spe-cific process was localized in the cervical spine in two patients, in the thoracic and thoracolumbar - in 38, in the lumbar and lumbosacral in 32 patients. Isolated lesions of one or two vertebrae were observed in four cas-es, contact destruction in 48, a combination of contact and isolated destruction at 15. Combination of MRI and X-ray methods broadens the notion of morphological changes in the spine, the stage of the tuberculous process, allows one to study the patterns of development And the dynamics of TC, the effectiveness of conservative and operative treatment
Informativity of magnetic-resonance tomography in diagnosis of tuberculosis spondilites and its complications89 magnetic resonance tomograms, which were performed by 72 patients with TS, were analyzed. A spe-cific process was localized in the cervical spine in two patients, in the thoracic and thoracolumbar - in 38, in the lumbar and lumbosacral in 32 patients. Isolated lesions of one or two vertebrae were observed in four cas-es, contact destruction in 48, a combination of contact and isolated destruction at 15. Combination of MRI and X-ray methods broadens the notion of morphological changes in the spine, the stage of the tuberculous process, allows one to study the patterns of development And the dynamics of TC, the effectiveness of conservative and operative treatment
Journal problems of biology and medicine -
 В теле человека насчитывается около 600 лимфатических узлов, однако в норме пальпаторно могут определяться только подчелюстные, подмышечные и паховые лимфоузлы
В теле человека насчитывается около 600 лимфатических узлов, однако в норме пальпаторно могут определяться только подчелюстные, подмышечные и паховые лимфоузлы -
 In the combined course of tuberculosis with HIV infection, the leading clinical manifestations of coinfection were asthenovegetative, bronchopulmonary syndromes, lesions of the skin and mucous membranes, lymphadenopathy, hepatomegaly, and weight loss. The structure of clinical forms of tuberculosis and its clinical manifestations largely depend on the primary infection with Mycobacterium tuberculosis or HIV. The severity of the comorbid condition is largely determined by the clinical form of tuberculosis disease and the stage of HIV infection. Timely diagnosis of HIV-ТВ co-infcction and adequate management of patients slow down the rate of development of infectious processes of both infections, and have a positive effect on reducing the intensity of the epidemic process of both HIV infection and tuberculosis
In the combined course of tuberculosis with HIV infection, the leading clinical manifestations of coinfection were asthenovegetative, bronchopulmonary syndromes, lesions of the skin and mucous membranes, lymphadenopathy, hepatomegaly, and weight loss. The structure of clinical forms of tuberculosis and its clinical manifestations largely depend on the primary infection with Mycobacterium tuberculosis or HIV. The severity of the comorbid condition is largely determined by the clinical form of tuberculosis disease and the stage of HIV infection. Timely diagnosis of HIV-ТВ co-infcction and adequate management of patients slow down the rate of development of infectious processes of both infections, and have a positive effect on reducing the intensity of the epidemic process of both HIV infection and tuberculosis -
 Алгоритм диагностики туберкулеза периферических лимфатических узлов у ВИЧ - инфицированных детейВИЧ-инфекция - самый важный фактор риска развития туберкулеза. По данным Всемирной Организации Здравоохранения более 42 млн людей на планете живут сегодня с вирусом иммунодефицита человека, и каждый день эта цифра увеличивается еще на 14000-15000. Более 16 млн из этих людей больны туберкулезом. Около 95% больных двойной инфекцией являются жителями развивающихся стран. В странах с высокой инфицированностью населения ВИЧ у 30-50% больных ВИЧ-инфекцией развивается туберкулез и при этом резко растет смертность от заболевания, достигая 90%.
Алгоритм диагностики туберкулеза периферических лимфатических узлов у ВИЧ - инфицированных детейВИЧ-инфекция - самый важный фактор риска развития туберкулеза. По данным Всемирной Организации Здравоохранения более 42 млн людей на планете живут сегодня с вирусом иммунодефицита человека, и каждый день эта цифра увеличивается еще на 14000-15000. Более 16 млн из этих людей больны туберкулезом. Около 95% больных двойной инфекцией являются жителями развивающихся стран. В странах с высокой инфицированностью населения ВИЧ у 30-50% больных ВИЧ-инфекцией развивается туберкулез и при этом резко растет смертность от заболевания, достигая 90%.
Инновационные подходы к диагностике, лечению и профилактике туберкулеза и неспецефической респираторной патологии у взрослых и детей -
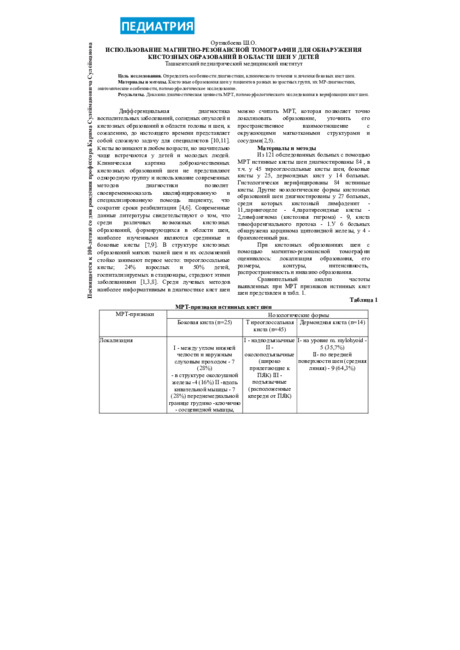 Использование магнитно-резонансной томографии для обнаружения кистозных образований в области шеи у детейОпределить особенности диагностики, клинического течения и лечения боковых кист шеи.
Использование магнитно-резонансной томографии для обнаружения кистозных образований в области шеи у детейОпределить особенности диагностики, клинического течения и лечения боковых кист шеи.
Pediatrics -
 Performance evaluation of pulse therapy in patients with systemic lupus erythematosusThe work was carried out examination and treatment of 30 patients with systemic lupus erythematosus (SLE). All patients underwent synchronous intensive therapy (SIT), which included a three-fold plasmapheresis (PF) with removal of 40-60 ml of plasma per kg of patient weight at intervals of 4-5 days. After each PF intra-venously over 45 minutes was administered 1.0 MP, and after the second - more added 1.0 cyclophosphamide. The dose of oral prednisolone should not exceed 40 mg / day. In the second phase was introduced on a monthly basis only 1.0 cyclophosphamide. Significantly decreased the frequency of erythema in the form of "butterfly", stomatitis, cheilitis enantemy and lupus, edema syndrome. Completely regressed pulmonary process, fever, lymphadenopathy, stabilized body weight, less defined polyserositis, arthritis
Performance evaluation of pulse therapy in patients with systemic lupus erythematosusThe work was carried out examination and treatment of 30 patients with systemic lupus erythematosus (SLE). All patients underwent synchronous intensive therapy (SIT), which included a three-fold plasmapheresis (PF) with removal of 40-60 ml of plasma per kg of patient weight at intervals of 4-5 days. After each PF intra-venously over 45 minutes was administered 1.0 MP, and after the second - more added 1.0 cyclophosphamide. The dose of oral prednisolone should not exceed 40 mg / day. In the second phase was introduced on a monthly basis only 1.0 cyclophosphamide. Significantly decreased the frequency of erythema in the form of "butterfly", stomatitis, cheilitis enantemy and lupus, edema syndrome. Completely regressed pulmonary process, fever, lymphadenopathy, stabilized body weight, less defined polyserositis, arthritis
Journal problems of biology and medicine -
 ASSESSMENT OF DANGERS FOR CHILDREN AND ADOLESCENTS WHO ARE HOUSEHOLD CONTACT OF TUBERCULOSIS INFECTIONIn article is evaluated danger household contact of tuberculous infection in development of the disease of children and adolescents in Samarkand state antituberculosis dispensary. Often in family tuberculosis was ill the mother, in most cases noted contact with the mother. In general, children and adolescents are infected as result of contact with disseminated form tuberculosis patients. The risk of the development tuberculosis of children, increased if the source of infections was earlier in prison zone. The negative social factors are considered as the prognostic factor to epidemic tension. The danger of the disease tuberculosis increases of children and adolescents from household centre tuberculosis, in which mother or two members of families (the close relatives) seek with tuberculosis. The children have a high danger of the development of the disease and particularly need for observation and undertaking preventive sanitary action.
ASSESSMENT OF DANGERS FOR CHILDREN AND ADOLESCENTS WHO ARE HOUSEHOLD CONTACT OF TUBERCULOSIS INFECTIONIn article is evaluated danger household contact of tuberculous infection in development of the disease of children and adolescents in Samarkand state antituberculosis dispensary. Often in family tuberculosis was ill the mother, in most cases noted contact with the mother. In general, children and adolescents are infected as result of contact with disseminated form tuberculosis patients. The risk of the development tuberculosis of children, increased if the source of infections was earlier in prison zone. The negative social factors are considered as the prognostic factor to epidemic tension. The danger of the disease tuberculosis increases of children and adolescents from household centre tuberculosis, in which mother or two members of families (the close relatives) seek with tuberculosis. The children have a high danger of the development of the disease and particularly need for observation and undertaking preventive sanitary action.
Journal of Cardiorespiratory Research -
 По данным ВОЗ, в настоящее время на Земле имеется 20-30 млн. больных активным туберкулезом всех локализаций. Ежегодно заболевают вновь до 9 миллионов, а умирают около 1,42 миллионов человек. [1].
По данным ВОЗ, в настоящее время на Земле имеется 20-30 млн. больных активным туберкулезом всех локализаций. Ежегодно заболевают вновь до 9 миллионов, а умирают около 1,42 миллионов человек. [1]. -
 Leishmaniasis is one of the most important medical and social problems in dermatology. The article presents literature data of leishmaniasis, a disease that is endemic in the Central Asian region. Dermatologists should have a certain caution about the development of this disease, especially in the autumn period due to the widespread migration of the population. The main forms of leishmaniasis and its clinical symptoms are described. Attention is paid to the rarely occurring tubercle form of cutaneous leishmaniasis. A clinical case of tubercle form, confirmed by histological examination and other methods, is also presented.
Leishmaniasis is one of the most important medical and social problems in dermatology. The article presents literature data of leishmaniasis, a disease that is endemic in the Central Asian region. Dermatologists should have a certain caution about the development of this disease, especially in the autumn period due to the widespread migration of the population. The main forms of leishmaniasis and its clinical symptoms are described. Attention is paid to the rarely occurring tubercle form of cutaneous leishmaniasis. A clinical case of tubercle form, confirmed by histological examination and other methods, is also presented. -
 Прогнозирование риска развития туберкулезного менингитаТуберкулез ЦНС, особенно туберкулёзный менингит (ТМ) сегодня, как и в прошлые времена, является одним из наиболее трудно диагностируемых заболеваний. Современное его выявление (в срок 10-12 дней) наблюдается лишь у 20-30% больных, что объясняется многообразием его клинических и морфологических проявлений. Проблема туберкулезного менингита - это проблема поздней диагностики и, как следствие, несвоевременно назначенной терапии, что приводит к неблагоприятным исходам в виде инвалидизации или смерти больных.
Прогнозирование риска развития туберкулезного менингитаТуберкулез ЦНС, особенно туберкулёзный менингит (ТМ) сегодня, как и в прошлые времена, является одним из наиболее трудно диагностируемых заболеваний. Современное его выявление (в срок 10-12 дней) наблюдается лишь у 20-30% больных, что объясняется многообразием его клинических и морфологических проявлений. Проблема туберкулезного менингита - это проблема поздней диагностики и, как следствие, несвоевременно назначенной терапии, что приводит к неблагоприятным исходам в виде инвалидизации или смерти больных.
Инновационные подходы к диагностике, лечению и профилактике туберкулеза и неспецефической респираторной патологии у взрослых и детей -
 Estimation of efficiency of application of minimally invasive technologies in diagnostics and treatment of tuberculosis obstructive forms of the urinary waysPercutaneous nephrostomy and stenting for tuberculosis of the kidneys with supravesical obstruction creates the conditions for normalizing the passage of urine. The accumulated experience allows us to positively assess the role of PKNS as a method of choice for the release and assessment of the reserves of renal function against the background of tuberculous changes in the upper urinary tract, and stenting for tuberculosis of the kidneys with supravesical obstruction creates the conditions for normalizing the passage of urine.
Estimation of efficiency of application of minimally invasive technologies in diagnostics and treatment of tuberculosis obstructive forms of the urinary waysPercutaneous nephrostomy and stenting for tuberculosis of the kidneys with supravesical obstruction creates the conditions for normalizing the passage of urine. The accumulated experience allows us to positively assess the role of PKNS as a method of choice for the release and assessment of the reserves of renal function against the background of tuberculous changes in the upper urinary tract, and stenting for tuberculosis of the kidneys with supravesical obstruction creates the conditions for normalizing the passage of urine.
Doctor's Herald -
 Quality of children and adolescents life with pulmonary tuberculosis depend- Ing on existence of the accompanying pathologyWork is devoted to studying of life quality parameters of children and adolescents with tuberculosis. Laboratory and instrumental methods examination of patients do not cover all aspect of tuberculous infection and do not allow valuing the condition of children and adolescents with pulmonary tuberculosis. At analysis of life’s quality there is full possibility to define the influence of the disease on physical, psychological and social aspects of the organism’s functioning. The analysis of quantitative indexes children and adolescents quality of life was conducted depending on accompanying pathology. For research was used the questionnaire of Pediatric Quality of Life Inventory - PedsQL. Questionnaire of PedsQL 4.0. includes 23 questions, incorporated in 4 scales. Every question has 5 variants of answers: "no", "hardly ever", "sometimes", "often" and "almost always", from which it is needed to choose one, most going near a situation.
Quality of children and adolescents life with pulmonary tuberculosis depend- Ing on existence of the accompanying pathologyWork is devoted to studying of life quality parameters of children and adolescents with tuberculosis. Laboratory and instrumental methods examination of patients do not cover all aspect of tuberculous infection and do not allow valuing the condition of children and adolescents with pulmonary tuberculosis. At analysis of life’s quality there is full possibility to define the influence of the disease on physical, psychological and social aspects of the organism’s functioning. The analysis of quantitative indexes children and adolescents quality of life was conducted depending on accompanying pathology. For research was used the questionnaire of Pediatric Quality of Life Inventory - PedsQL. Questionnaire of PedsQL 4.0. includes 23 questions, incorporated in 4 scales. Every question has 5 variants of answers: "no", "hardly ever", "sometimes", "often" and "almost always", from which it is needed to choose one, most going near a situation.
Doctor's Herald -
THE ROLE OF OSTEOREPLACEMENT MATERIALS IN RECONSTRUCTIVE SURGERY FOR SPINAL TUBERCULOSIS
European International Journal of Multidisciplinary Research and Management StudiesThe study is based on data from a survey of 658 patients with osteoarticular tuberculosis, which was performed in 482 (73.3%) cases of radical reconstructive surgery (RVO) of the spine. Of 482 patients with spinal tuberculosis, in 461 (95.6%) cases, RVO was using a titanium mesh cage (Piramesh), and in 21 (4.4%) patients using the traditional-classical method with autobone fusion.
To fill the lumen of the titanium mesh cage, it is rational to use autologous crumbs, collapAn and hydroxyapatite compounds. In case of tuberculosis of large joints, to restore the function and defect of bones, total joint arthroplasty is a solution to a serious problem.