





Биология ва тиббиёт муаммолари, 2014, №4.1 (81)
103
UDC:
616.72-002:615.831
INDEX CHANGES QUALITY OF LIFE IN PATIENTS WITH OSTEOARTHRITIS IN THE
ELDERLY AGE AFTER THE SANATORIUM STAGE OF REHABILITATION
T.G. BAKALYUK
HSEI “I.Ya. Gorbachevsky Ternopil State Medical University of Ministry
of Public Health of Ukraine”
Resume.
In the study quality of life
in elderly patients
with osteoarthritis
using international
EuroQol
questionnaire
were obtained
substantiated data about positive
impact
of
spa treatment
on
quality
of life
by
given
group of patients
compared with
outpatient treatment.
Multidisciplinary
nature
of medical
rehabilitation
in spa
conditions
, using a wide
range
of rehabilitation
methods
promotes more
complex
influence on an organism and
allows to save
remission
for murch longer term.
Key words:
quality of life
, spa
treatments
, osteoarthritis.
ИНДЕКС ИЗМЕНЕНИЯ КАЧЕСТВА ЖИЗНИ У БОЛЬНЫХ ОСТЕОАРТРОЗОМ В
ПОЖИЛОМ ВОЗРАСТЕ ПОСЛЕ САНАТОРНОГО ЭТАПА РЕАБИЛИТАЦИИ
Т.Г. БAKAЛЮK
ГВУЗ «Тернопольский Государственный медицинский университет
им. И.Я. Горбачевского МЗ Украины»
Резюме.
В качестве исследования жизни пожилых пациентов с остеоартрозом с
использованием международной анкеты EuroQoL были получены обоснованные данные о
положительном влиянии курортного лечения на качество жизни по данной группе больных, по
сравнению с амбулаторным лечением. Междисциплинарный характер медицинской реабилитации
в определенных условиях, используя широкий спектр методов реабилитации способствует более
комплексное воздействие на организм и позволяет сохранить ремиссии в долгосрочной
перспективе.
Ключевые слова:
качество жизни, процедуры, остеоартрит.
Introduction.
Osteoarthritis (OA) is one of
the most common disorders of the muscle-skeletal
system, especially in the elderly age group ( in every
third elderly person, reaching 70% among those
who have over 65 years). During the natural aging
occurs involutional changes in the connective tissue,
especially in the tendons, ligaments, cartilage, bone
tissue, in the walls of blood vessels, muscles [2].
Thus aging of div contributes to the accumulation
of diseases. During the examination in elderly and
senile patients were diagnosed from three to five
different diseases. Modern elderly person is - a
unique clinical phenomenon from the point of view
on availability and the combination of its diverse in
character and course of diseases that are competing
for their prognostic significance and impact on
quality of life. OA attributed to diseases with high
comorbidity, and founded that patients with OA
have a significantly higher risk of comorbid
conditions than patients who do not suffering from
OA [4].
Clinical
experience
and
numerous
publications data suggest that OA is often associated
with subsequent somatic disorders: hypertension,
coronary heart disease, obesity, diabetes, lung
diseases (chronic obstructive pulmonary disease)
and gastro- intestinal tract diseases. The greatest
burden on society observed in cases of combination
OA and osteodeficiency (osteopenia, osteoporosis
(OP)), which significantly decreses the quality of
life [5].
Quality of life
-
integrated
description
of
physical,
psychological, emotional
and
social
functioning of
a person
based on its subjective
perception
.
Assessment of quality of
life
at modern
stage
have more increasing
strong position
in
medicine
, reflecting
on the one
hand, the presence
of new medical
technologies that
do not affect the
life expectancy,
but significantly
improve
its
quality
, and from the other hand
- expanding
activity of
the patient,
increasing of its role in
choice
of methods
of diagnostic and
treatment [
9].
When selecting the questionnaires it is
important to consider that to be used in a clinical
studying suitable only those that give results of the
evaluation quality of life in a form of a single
summary score from 0 to 1.0. These includes a
generic questionnaire EQ-5D (EuroQol) [8]. This
general questionnaire is easy to fill , widely used in
different countries and gives during the processing

Index changes quality of life in patients with osteoarthritis in the elderly age after the sanatorium stage of…
104
Проблемы биологии и медицины, 2014, №4.1 (81)
of collected data single score to measure the quality
of life, represented by values between 0 and 1,
which also provides the possibility of its using in
clinical trials. This questionnaire is widely used in
various clinical situations , including in assessing
the quality of life patients with rheumatic diseases
[7].
The aging process is controversial, because
on the background of regression processes - atrophy,
degradation, etc., develops progressive trends of
creating
the
new
compensatory-adaptive
mechanisms to maintain homeostasis in an aging
div, which, however, does not fully offset the
growing phenomena of degradation [2]. It should be
noted that the adaptive capacity of the aging div is
reduced, the possibility of development various
diseases increases. In this context, particularly
important in cases of illness in the elderly patient is
the role
of sanogenetic
mechanisms,
their
stimulation and support. A special interest belongs
to the sanatorium stage of rehabilitation, whose
mission is the prevention of disease progression,
stimulation of compensatory capacity of the muscle-
skeletal system and the possible restoration of joint
function. Spa treatment has a special place in the
treatment and preventive care of elderly patients, as
a stage in the system of rehabilitation of many
chronic diseases. Multi-disciplinary nature of
medical rehabilitation in spa conditions, a wide
range of rehabilitation methods can embrace
patients of all age groups with the most common
diseases [1].
Compared with medication treatment,
natural and artificial physical factors, when they are
properly used, characterized by the absence of
allergies, lower incidence and severity of side
effects, the ability of positively influencing on the
number of pathological processes and the whole
div, thus helping to improve the quality of life and
are important in the prevention of premature aging
[2]. In the resort conditions further rehabilitation is
indicated for patients with initial stages of OA,
disabled (groups I and II), patients with resistant
synovitis and comorbidity with the possibility of
self-servicing (including general contraindications
for a spa treatment) [3].
The aim of the study. To investigate the
quality of life in elderly patients with osteoarthritis
using international EuroQol questionnaire to
evaluate the effectiveness of spa treatment.
Materials and methods. In study were
included 72 patients aged from 60 to 78 years,
middle age was 67,6 ± 8,7 years. Among the
patients predominates women - 88.4 %. I
radiographic stage of osteoarthritis by J.H. Kellgren-
Lawrence [ 6] was diagnosed in 23,3 % of patients ,
II stage - in 76,7 %. In the view of modern geriatric
approaches applying of the physical factors in
patients with OA who were in the spa rehabilitation
stage in the appointment of balneotherapeutic
procedures we gave preference to ultrasonic
inhalation of mineral waters and baths, from
physiotherapy usually prescribed magnetic-lazer
therapy,
interferential
therapy,
patients
also
performed massage and physical rehabilitation . In
order
to
prevent
climate-adaptational
and
reaclimate-adaptational reactions and optimization
process of climate-adaptation were included into the
treatment complex (based on established risk
factors) adaptogens and treatment procedures that
have adaptogenic action (phytoaeroionisation ,
singlet-oxygen therapy). In the process of
rehabilitation treatment in sanatorium conditions ,
we have selected the most effective combination of
different methods of rehabilitation, which caused
the most significant treatment effectiveness: a
combination of balneotherapy, physiotherapy and
exercise therapy. To improve continuity during
medical rehabilitation, at discharging from the
sanatorium patients were given written (in the form
of special attractions) recommendatitons about
further treatment, lifestyle, physical activity, diet
etc. By the method of randomization, patients were
divided into two groups. A marked difference for
the main source of clinical and functional
parameters between the groups were not observed.
The control group consisted of 14 patients of the
same age without joint pathology. Treatment
regimens differed between the studying groups the
presence in one of the groups sanatorium stage of
rehabilitation. In the first group (n=34) patients
received Structum 500 mg 2 times a day ( within 6
months of the year ) and courses of NSAID,
including mainly patients treated with meloxicam
(at a dose of 7,5 mg/d) or nimesulide (in dose of
100-200 mg/d) for 7-10 days during worcening. The
patients of the second group (n=38) during the 18-
21 day were on spa treatment (once a year ), in the
scheme of rehabilitation were: sitting hydrogen
sulfide baths, a concentration of 80 mg/L for 10
minutes at a temperature of 36
0
C , the course of 8
procedures every other day or ultrasonic inhalation
by hydrogen sulfide water, period of 5 minutes; blue
clay applications every other day at 26
0
C
temperature; interferential therapy and magnet-lazer
therapy on the affected joints to 8 treatments
alternately every other day; pneumomassage; classes
of physical rehabilitation therapy, aromatherapy,
singlet -oxygen therapy . After the sanatorium stage
of rehabilitation patients are taking drugs containing
chondroitin sulfate (within 6 months of the year), at
worcening of NSAIDs.
Assessment quality of life related to health ,
was conducted using an international EuroQol-5D-
European Quality of Life instrument (EQ-5D),

T.G. Bakalyuk
Биология ва тиббиёт муаммолари, 2014, №4.1 (81)
105
which consists of two parts. At first part the patient
self- assessed his condition by 5 parameters:
mobility, self-care, usual activities, pain and
discomfort, anxiety and depression. In each variant
patients could give three possible answers : No
problem - 1, there is some problem - 2, much of the
problem - 3. In the second part of the questionnaire ,
patients assessed their health on a scale from 0 to
100 on the VAS, the so-called thermometer , where
0 means the worst condition , 100 - the best state of
health of the patient. This part of the questionnaire
is a quantitative assessment of general health.
Statistical analysis of the results was done in the
department of statistical system research at SHEE
"Ternopil State Medical University by I.Y.
Gorbachevsky Ministry of Health of Ukraine" in the
software
package
Statsoft
STATISTIC.
To
determine the reliability of the differences in the
change of certain indicators were used parametric
and non-parametric methods: criterion Wilkoksona,
two-sided
Fisher's
criterion.
A
significant
differences were considered when the degree of
probability of error-free prognosis is (p) 95% (p
<0.05).
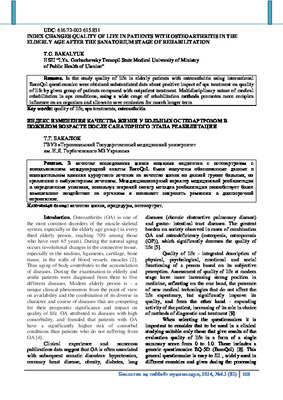
Table.
Dynamics of health status of patients with OA according to the EQ-5D questionnaire
Health status
The number of respondents of the first
group (n = 34)
The number of respondents of the
second group (n = 38)
At the beginning of
the study
After 12 months
At the beginning of
the study
After 12 months
абс.
%
абс.
%
абс.
%
абс.
%
Moving in space
No problem
3
8,8
5
14,7
2
5,2
15
39,4
There are some
problems
31
91.2
29
85,3
36
94,8
23
60,6
Not gets out of bed
0
0
0
0
0
0
0
0
Self-service
No problem
21
61,7
20
58,8
26
68,4
29
76,3
There are some
problems
13
38,3
14
41,2
12
31,6
9
23,7
Is unable to wash and
dress
0
0
0
0
0
0
0
0
Everyday activity
No problem
6
17,6
6
17,6
5
13,1
12
31,5
There are some
problems
24
70,5
22
64,7
30
78,9
26
68,5
Can not perform daily
activities
4
11,9
6
17,7
3
8,0
0
0
Pain and discomfort
No pain or discomfort
0
0
0
0
0
0
7
18,4
There is some pain and
discomfort
26
76,4
28
82,3
29
76,3
27
71,0
There is a lot of pain
and discomfort
8
23,6
6
17,7
9
23,7
4
10,6
Anxiety and depression
No anxiety and
depression
11
32,3
12
35,2
12
31,5
18
47,3
There is little anxiety
and depression
20
58,8
17
50,0
24
63,3
20
52,7
There are severe anxiety
and depression
3
8,9
5
14,8
2
5,2
0
0
Health status changes during the year
Improved
6
20,4
22
57,9
Not changed
20
56,1
16
42,1
Worsened
8
23,5
0
0

Index changes quality of life in patients with osteoarthritis in the elderly age after the sanatorium stage of…
106
Проблемы биологии и медицины, 2014, №4.1 (81)
Results and discussion. General description
of the health status of patients studied with OA
according to EQ-5D questionnaire is given in the
table.
In all patients with osteoarthritis were found
health problems of different severity degrees.
Mostly suffers ability to travel and daily activity.
This data confirms that the OA in the elderly age
reduces quality of life. After 12 months, according
to questionnaire, health status was different in two
groups . Reliable positive trend was in patients from
the second group 57,9 % (p < 0,05), as a result of
improving the ability to travel in space, reducing
pain and discomfort and increasing of daily activity.
According to the second part of the
questionnaire EQ-5D, at baseline, most patients had
reduced general health assessment: the first group to
51,91 ± 1,07 ( median for «thermometer» EQ 52
points) in the second group to 50,65 ± 1,17 ( median
48,5 points) in comparison with the best state of
possible health.
12 months after the sanatorium stage of
rehabilitation of patients with repeated testing were
produced the following results : The average index
quality of life on the "thermometer" EQ-5D
questionnaire in the first group of patients was 54,76
± 1,23 ( median - 56 points), the second group was
69,28 ± 0,89 (median - 70 points), reliability
differences is high : p < 0,001.
In the category quality of life most of all
patients reacted on the presence of sanatorium stage
of rehabilitation in the category "movement in
space" (GPA retesting 1,60 ± 0,08, p < 0,001),
"daily activity" ( GPA retesting 1 68 ± 0,07, p <
0,001), " pain / discomfort "(GPA retesting 1,92 ±
0,08, p < 0,001)," anxiety / depression (GPA
retesting 1 52 ± 0,08, p < 0,05).
Thus, the data suggested that in elderly
patients with OA who were once a year on a spa
treatment and took over 6 months structure-
modification drugs significantly upgraded quality of
life during 12 months.
Conclusions: 1. Based on the analysis were
founded that elderly patients with OA who
underwent rehabilitation treatment in sanatorium-
health resorts have continued improving quality of
life in comparison with patients who were treated
only in outpatient conditions.
2.
Availability
sanatorium
stage
of
rehabilitation in the treatment of elderly patients
with OA contributes more complex influence on the
human organism.
3. Multi-disciplinary nature of medical
rehabilitation in spa conditions, a wide range of
used restorative treatment methods can affect the
quality of life and maintain remission for more
longer period in comparison with outpatient
treatment.
4. Monitoring the quality of life can not only
control the functional state of the organism in the
elderly aged people at various stages of treatment ,
but also to properly evaluate the effectiveness of
treatment, and, if necessary, to carry out the
correction of rehabilitation activities.
Perspectives for future research. Aimed at
studying the impact of rehabilitative and preventive
measures on the quality of life in elderly patients
with osteoarthritis at other stages of rehabilitation.
Further work in this direction is reasonable and
economically justified.
References:
1.
Golyachenko A.O., Martynyuk V.I., Bakalyuk
T.G. Medical rehabilitation in the spa conditions //
Journal of research. - 2007 . - № 4. - P. 8-9.
2.
Kazymyrko V.K., KovalenkoV.N., Flehontova
V.V. Involutional osteoarthritis and osteoporosis. -
Donetsk: Publisher Zaslavsky A.J., 2011. - 724 p.
3.
Kovalenko
V.N.,
Bortkiewicz
A.P.
Osteoarthritis . Practical guidance . - K.: Moryon ,
2005. - 592 p.
4.
Mendel O.I., Naumov A.V., Alekseeva L.I. et
al Osteoarthritis as a factor of risk in cardio-vascular
catastrophes // Ukrainian Journal of Rheumatology .
- 2010 . - № 3. - P. 68-73.
5.
Povoroznyuk V.V. Osteoarthritis // Art of
treatments. - 2004 . - № 3. - P.16 -23.
6.
Altman R., Asch E., Bloch D. et al. The
American College of Rheumatology criteria for the
classification and reporting of osteoarthritis of the
knee // Arthritis Rheum. - 1986 . - № 29. - P. 1039-
1049 .
7.
Harrison M.J., Davies L.M., Bansback N.J. et
al. The comparative responsiveness of the EQ-5D
and SF-6D to change in patients with inflammatory
arthritis // Qual Life Res. - 2009 . - № 18. - P. 1195-
1205.
8.
Herdman M., Gudex C., Lloyd A., et al.
Development and preliminary testing of the new
five-level version of EQ-5D (EQ-5D-5L) // Qual
Life Res. - 2011 . - № 20 . - P. 1727-1736.
9.
Langley P., Muller-Schwefe G., Nicolaou A.,
Liedgens H., Pergolizzi J., Varrassi G. The societal
impact of pain in the European Union: health-related
quality of life and healthcare resource utilization // J.
Med Econ. - 2010 . - № 1. - P. 571-581.

T.G. Bakalyuk
Биология ва тиббиёт муаммолари, 2014, №4.1 (81)
107
РЕАБИЛИТАЦИЯНИНГ САНАТОР
БОСҚИЧИДАН СЎНГ ОСТЕОАРТРОЗ
БИЛАН ОҒРИГАН ҚАРИЯЛАР ХАЁТ
ТАРЗИНИНГ ЎЗГАРИШ ИНДЕКСИ
Т.Г. БAKALЮK
Украина ССВ И.Я. Горбачевский номидаги
Тернополь Давлат медицина университети
Резюме.
EuroQoL халқаро анкетасини
қуллаган холда остеоартроз билан оғриган
қариялар хаёти текширилди. Бунинг натижасида,
ушбу гуруҳдаги беморлар хаёт тарзи амбулатор
даволаниш
билан
таққосланганда
курорт
даволанишнинг ижобий таъсири тўғрисида
асосланган
маълумотлар
олинди.
Тиббий
реабилитация
маълум
бир
шароитида
ребилитация усулларини кенг доирада қуллаш
орқали организмга комплекс таъсир кўрсатади
ва узоқ вақтга ремиссия босқичини сақлаб
қолади.
Калит сўзлар:
хаёт тарзи, муолажалар,
остеоартрит.