Library search
Search Results
-
 ASSESSMENT OF THE STATE OF LOCAL IMMUNE OF THE ORAL CAVITY IN PATIENTS WITH ACUTE PURULENT ODONTOGENIC OSTITISObjective: To study the characteristic features of local and systemic immunity in patients with acute purulent odontogemc ostitis of the jaw. Material and methods: The data obtained during the examination and treatment of 42 patients aged from 7 to 9 years with acute purulent odontogenic ostitis who applied to the TGSI clinic were analyzed. Results: Bacteriological study of wound discharge inpatients with acute purulent odontogenic ostitis showed that staphylococcus form the basis of microflora in species ratio. These microorganisms accounted for 82% of the total number of isolated strains. Conclusions: in acute purulent odontogenic ostitis, the ability of periodontal cells to recover is not observed, but rather the development of irreversible processes occurs, whichrequires surgical intervention and appropriate pharmacological correction.
ASSESSMENT OF THE STATE OF LOCAL IMMUNE OF THE ORAL CAVITY IN PATIENTS WITH ACUTE PURULENT ODONTOGENIC OSTITISObjective: To study the characteristic features of local and systemic immunity in patients with acute purulent odontogemc ostitis of the jaw. Material and methods: The data obtained during the examination and treatment of 42 patients aged from 7 to 9 years with acute purulent odontogenic ostitis who applied to the TGSI clinic were analyzed. Results: Bacteriological study of wound discharge inpatients with acute purulent odontogenic ostitis showed that staphylococcus form the basis of microflora in species ratio. These microorganisms accounted for 82% of the total number of isolated strains. Conclusions: in acute purulent odontogenic ostitis, the ability of periodontal cells to recover is not observed, but rather the development of irreversible processes occurs, whichrequires surgical intervention and appropriate pharmacological correction.
Stomatologiya -
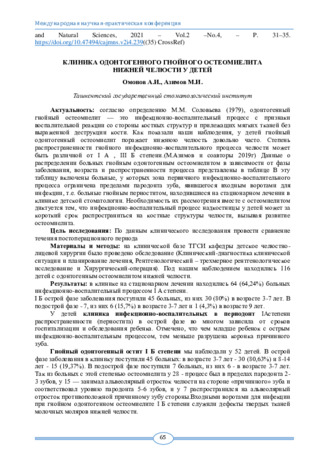 Клиника одонтогенного гнойного остеомиелита нижней челюсти у детей
Клиника одонтогенного гнойного остеомиелита нижней челюсти у детей
Topical issues of surgical dentistry and dental implantologyСогласно определению М.М. Соловьева (1979), одонтогенный гнойный остеомиелит — это инфекционно-воспалительный процесс с признаки воспалительной реакции со стороны костных структур и прилежащих мягких тканей без выраженной деструкции кости. Как показали наши наблюдения, у детей гнойный одонтогенный остеомиелит поражает нижнюю челюсть довольно часто. Степень распространенности гнойного инфекционно-воспалительного процесса челюсти может быть различной от I А , III Б степени.(М.Азимов и соавторы 2019г) Данные о распределении больных гнойным одонтогенным остеомиелитом в зависимости от фазы заболевания, возраста и распространенности процесса представлены в таблице В эту таблицу включены больные, у которых зона первичного инфекционно-воспалительного процесса ограничена пределами пародонта зуба, явившегося входным воротами для инфекции, т.е. больные гнойным периоститом, находившиеся на стационарном лечении в клинике детской стоматологии. Необходимость их рассмотрения вместе с остеомиелитом диктуется тем, что инфекционно-воспалительный процесс надкостницы у детей может за короткий срок распространиться на костные структуры челюсти, вызывая развитие остеомиелита.
-
 The possibility of using ultrasound osteometry for the diagnosis of acute odontogenic osteitis and osteomyelitis of the jaws was studied. The study was conducted in 43 children, of which 14 children and 15 adults had heterogeneous abscesses and phlegmon. Acute odontogenic osteitis - in 11 children and 11 adults, acute odontogenic osteomyelitis - mil children and 11 adults. The studies were carried out using an ultrasonic diagnostic device with an EOM-Olts echoosteometer. in 1-3 and 7-10 days. The speed of ultrasound m the jaw was calculated by the formula C = L /1. The decrease in the speed of ultrasound in the jaw bone and its dependence on the forms of the inflammatory process. Ultrasonic osteometry allows bone pathology, to predict the course of the disease. Harmlessness, painlessness, ease of use. the ability to recommend echoosteometry for the diagnosis of pathological processes of the jaw in practical dentistry.
The possibility of using ultrasound osteometry for the diagnosis of acute odontogenic osteitis and osteomyelitis of the jaws was studied. The study was conducted in 43 children, of which 14 children and 15 adults had heterogeneous abscesses and phlegmon. Acute odontogenic osteitis - in 11 children and 11 adults, acute odontogenic osteomyelitis - mil children and 11 adults. The studies were carried out using an ultrasonic diagnostic device with an EOM-Olts echoosteometer. in 1-3 and 7-10 days. The speed of ultrasound m the jaw was calculated by the formula C = L /1. The decrease in the speed of ultrasound in the jaw bone and its dependence on the forms of the inflammatory process. Ultrasonic osteometry allows bone pathology, to predict the course of the disease. Harmlessness, painlessness, ease of use. the ability to recommend echoosteometry for the diagnosis of pathological processes of the jaw in practical dentistry. -
The possibility of using ultrasound osteometry for the diagnosis of acute odontogenic osteitis and osteomyelitis of the jaws was studied. The study was conducted in 43 children, of which 14 children and 15 adults had heterogeneous abscesses and phlegmon. Acute odontogenic osteitis - in 11 children and 11 adults, acute odontogenic osteomyelitis - in 11 children and 11 adults. The studies were carried out using an ultrasonic diagnostic device with an EOM-01ts echoosteometer. in 1-3 and 7-10 days. The speed of ultrasound in the jaw was calculated by the formula C = L / t. The decrease in the speed of ultrasound in the jaw bone and its dependence on the forms of the inflammatory process. Ultrasonic osteometry allows bone pathology, to predict the course of the disease. Harmlessness, painlessness, ease of use, the ability to recommend echoosteometry for the diagnosis of pathological processes of the jaw in practical dentistry.
-
 Assessment of the state of local immunity of the oral cavity in patients with acute purulent odontogenic osteitis
Assessment of the state of local immunity of the oral cavity in patients with acute purulent odontogenic osteitis
in LibraryTo study the characteristic features of local and systemic immunity in patients with acute purulent odontogenic ostitis of the jaw. Material and methods: The data obtained during the examination and treatment of 42 patients aged from 7 to 9 years with acute purulent odontogenic ostitis who applied to the TGSI clinic were analyzed.Results: Bacteriological study of wound discharge in patients with acute purulent odontogenic ostitis showed that staphylococcus form the basis of microflora in species ratio. These microorganisms accounted for 82% of the total number of isolated strains. Conclusions: in acute purulent odontogenic ostitis, the ability of periodontal cells to recover is not observed, but rather the development of irreversible processes occurs, which requires surgical intervention and appropriate pharmacological correction.
-
 ASSESSMENT OF HEMATOLOGICAL BLOOD PARAMETERS IN PRACTICALLY HEALTHY INDIVIDUALS AND PATIENTS WITH ACUTE PURULENT ODONTOGENIC OSTITISTo study the characteristic features of the cellular composition of blood in patients with acute purulent odontogenic ostitis of the jaw. Material and methods: The data obtained during the examination and treatment of 42 patients with acute purulent odontogenic ostitis at the age of 7 to 9 years, who apphed to the TGSI clinic, were studied. Results: In the patients, the indices of the red part of the blood were significantly lower than in the comparison group. A low level of hemoglobin can cause hemic tissue hypoxia and affect the state of the acid-base state of the blood, expressed in the form of acidosis, which activates anaerobic glycolysis. An increase in the level of lactic acid m cells can be one of the reasons for the disruption of local microcirculation and the accumulation of endogenous toxins. Conclusions: This pathology' is accompanied by a shift m the indicators of the white part of the blood, the observed hemic hypoxia leads to an increase in the level of lactic acid in the cells, which may be one of the reasons for the disruption of local microcirculation and the accumulation of endogenous toxins.
ASSESSMENT OF HEMATOLOGICAL BLOOD PARAMETERS IN PRACTICALLY HEALTHY INDIVIDUALS AND PATIENTS WITH ACUTE PURULENT ODONTOGENIC OSTITISTo study the characteristic features of the cellular composition of blood in patients with acute purulent odontogenic ostitis of the jaw. Material and methods: The data obtained during the examination and treatment of 42 patients with acute purulent odontogenic ostitis at the age of 7 to 9 years, who apphed to the TGSI clinic, were studied. Results: In the patients, the indices of the red part of the blood were significantly lower than in the comparison group. A low level of hemoglobin can cause hemic tissue hypoxia and affect the state of the acid-base state of the blood, expressed in the form of acidosis, which activates anaerobic glycolysis. An increase in the level of lactic acid m cells can be one of the reasons for the disruption of local microcirculation and the accumulation of endogenous toxins. Conclusions: This pathology' is accompanied by a shift m the indicators of the white part of the blood, the observed hemic hypoxia leads to an increase in the level of lactic acid in the cells, which may be one of the reasons for the disruption of local microcirculation and the accumulation of endogenous toxins.
Stomatologiya -
 Evaluation of hematological blood parameters in practically healthy individuals and patients with acute purulent odontogenic osteitis
Evaluation of hematological blood parameters in practically healthy individuals and patients with acute purulent odontogenic osteitis
in LibraryTo study the characteristic features of the cellular composition of blood in patients with acute purulent odontogenic ostitis of the jaw. Material and methods: The data obtained during the examination and treatment of 42 patients with acute purulent odontogenic ostitis at the age of 7 to 9 years, who applied to the TGSI clinic, were studied. Results: In the patients, the indices of the red part of the blood were significantly lower than in the comparison group. A low level of hemoglobin can cause hemic tissue hypoxia and affect the state of the acid-base state of the blood, expressed in the form of acidosis, which activates anaerobic glycolysis. An increase in the level of lactic acid in cells can be one of the reasons for the disruption of local microcirculationand the accumulation of endogenous toxins. Conclusions: This pathology is accompanied by a shift in the indicators of the white part of the blood, the observed hemic hypoxia leads to an increase in the level of lactic acid in the cells, which may be one of the reasons for the disruption of local microcirculation and the accumulation of endogenous toxins.
-
 Assessment of the Status of Local Immunity in Patients with Acute Purulent Odontogenic by Osteitis of the Jaw
Assessment of the Status of Local Immunity in Patients with Acute Purulent Odontogenic by Osteitis of the Jaw
in LibraryThe aim of this study was to study the characteristic features of local and systemic immunity in patients with acute purulent odontogenicostitis of the jaw. We examined 38 patients with acute purulent odontogenicperiostitis, who applied to the TSSI clinic. Clinical hematological immunological research methods were used. It was revealed that the most frequent associations of microorganisms in acute purulent odontogenicostitis of the jaws are Staphylococcus aureus, Staphylococcus epidermicus, registered in more than half of the cases. There was an increase in immunoglobulin G in the blood in acute purulent odontogenicostitis.
-
 Assessment of the Status of Local Immunity in Patients with Acute Purulent Odontogenic by Osteitis of the Jaw
Assessment of the Status of Local Immunity in Patients with Acute Purulent Odontogenic by Osteitis of the Jaw
in LibraryThe aim of this study was to study the characteristic features of local and systemic immunity in patients with acute purulent odontogenicostitis of the jaw. We examined 38 patients with acute purulent odontogenicperiostitis, who applied to the TSSI clinic. Clinical hematological immunological research methods were used. It was revealed that the most frequent associations of microorganisms in acute purulent odontogenicostitis of the jaws are Staphylococcus aureus, Staphylococcus epidermicus, registered in more than half of the cases. There was an increase in immunoglobulin G in the blood in acute purulent odontogenicostitis.
-
 Острое воспаление слизистой оболочки среднего уха — слуховой трубы, барабанной полости и клеток сосцевидного отростка — заболевание, наиболее распространенное в детском возрасте, является многоплановой проблемой. Острый средний отит (ОСО) у ВИЧ-инфицированных детей относится к неотложной патологии и требует внимания не только оториноларингологов. но и педиатров, детских инфекционистов, аллергологов. Так, в классификации, предложенной М.Я. Козловым (1, 3, 4, 10), выделен «явный острый средний отит», «острый средний отит при инфекционных заболеваниях»,«экссудативно-аллергический рецидивирующий средний отит».
Острое воспаление слизистой оболочки среднего уха — слуховой трубы, барабанной полости и клеток сосцевидного отростка — заболевание, наиболее распространенное в детском возрасте, является многоплановой проблемой. Острый средний отит (ОСО) у ВИЧ-инфицированных детей относится к неотложной патологии и требует внимания не только оториноларингологов. но и педиатров, детских инфекционистов, аллергологов. Так, в классификации, предложенной М.Я. Козловым (1, 3, 4, 10), выделен «явный острый средний отит», «острый средний отит при инфекционных заболеваниях»,«экссудативно-аллергический рецидивирующий средний отит». -
 Гнойный холангит: частота и причины их возникновения, классификация, диагностика и хирургическая тактикаГнойный холангит (ГХ) – это одно из наиболее частых и тяжелых осложнений доброкачественных и злокачественных заболеваний желчных путей. Проявляющимся комплексом органических и функциональных, общих и местных патологических изменений в организме в результате развития инфекционного процесса в желчных протоках, вызванных нарушением их проходимости.
Гнойный холангит: частота и причины их возникновения, классификация, диагностика и хирургическая тактикаГнойный холангит (ГХ) – это одно из наиболее частых и тяжелых осложнений доброкачественных и злокачественных заболеваний желчных путей. Проявляющимся комплексом органических и функциональных, общих и местных патологических изменений в организме в результате развития инфекционного процесса в желчных протоках, вызванных нарушением их проходимости.
Journal problems of biology and medicine -
 Цитологические показатели эффективности лечения острого гнойного одонтогенного периостита челюстей с использованием салфеток «активтекс»Актуальность исследования. Острый гнойный одонтогенный периостит челюстей представляет актуальную проблему в стоматологии и челюстнолицевой хирургии. В последние годы, как в поликлинических стоматологических учреждениях, так и в челюстнолицевых стационарах отмечено увеличение больных с данной патологией до 40 % [2, 6]. Возросла тяжесть острого гнойного одонтогенного периостита челюстей , которая нередко приводит к возникновению воспалительных осложнений, таких как абсцессы и флегмоны лица и шеи, одонтогенные остеомиелиты, одонтогенные верхнечелюстные синуситы, мсдиастсниты, сепсис и др. [3,6, 7,8,]. Известно, что в последние годы при лечении острых воспалительных заболеваний челюстнолицевой области большое внимание отводится, качеству дренирования, при недостаточном или неправильном дренировании гнойного очага возникают осложнения, которые усугубляют тяжесть основного заболевания, усложняют лечение, увеличивают сроки выздоров-лсния[1,4].
Цитологические показатели эффективности лечения острого гнойного одонтогенного периостита челюстей с использованием салфеток «активтекс»Актуальность исследования. Острый гнойный одонтогенный периостит челюстей представляет актуальную проблему в стоматологии и челюстнолицевой хирургии. В последние годы, как в поликлинических стоматологических учреждениях, так и в челюстнолицевых стационарах отмечено увеличение больных с данной патологией до 40 % [2, 6]. Возросла тяжесть острого гнойного одонтогенного периостита челюстей , которая нередко приводит к возникновению воспалительных осложнений, таких как абсцессы и флегмоны лица и шеи, одонтогенные остеомиелиты, одонтогенные верхнечелюстные синуситы, мсдиастсниты, сепсис и др. [3,6, 7,8,]. Известно, что в последние годы при лечении острых воспалительных заболеваний челюстнолицевой области большое внимание отводится, качеству дренирования, при недостаточном или неправильном дренировании гнойного очага возникают осложнения, которые усугубляют тяжесть основного заболевания, усложняют лечение, увеличивают сроки выздоров-лсния[1,4].
Doctor's Herald -
 Изучение этиологической характеристики среднего отита у детей
Изучение этиологической характеристики среднего отита у детей
Prospects for the development of medicineАктуальность проблемы воспалительной патологии среднего уха у детей обусловлена ее высокой распространенностью и вероятностью развития осложнений.Воспаление среднего уха встречается в любом возрасте, среди других заболеваний ЛОР-органов острый гнойный средний отит диагностируется в 20-30% случаев. Особенно часто заболевание наблюдается у детей первых лет жизни, являются из наиболее частых причин обращения за медицинской помощью, занимая лидирующую позицию в общей структуре ЛОР патологии.
-
 Влияние течения послеоперационного периода на состояние репродуктивного здоровья женщин перенесших перитонит в детском возрастеОстрый гнойный перитонит одно из грозных хирургических заболеваний детского возраста. Наиболее частой причиной его является острый деструктивный аппендицит. У девочек при этом в патологический процесс непосредственно вовлекаются матка и ее придатки. По статистическим данным аппендицит чаще встречается в пубертатном периоде, когда чувствитель- ность к патологическим воздействиям велика во всех звеньях половой системы, что еще более усугубляет проблему [1,2,7,9, 10,11,12].
Влияние течения послеоперационного периода на состояние репродуктивного здоровья женщин перенесших перитонит в детском возрастеОстрый гнойный перитонит одно из грозных хирургических заболеваний детского возраста. Наиболее частой причиной его является острый деструктивный аппендицит. У девочек при этом в патологический процесс непосредственно вовлекаются матка и ее придатки. По статистическим данным аппендицит чаще встречается в пубертатном периоде, когда чувствитель- ность к патологическим воздействиям велика во всех звеньях половой системы, что еще более усугубляет проблему [1,2,7,9, 10,11,12].
Journal problems of biology and medicine -
Investigated 45 young patients with acute myocardial infarction, divided three periods of mental disorders: acute, subacute and longterm effects. Found that in 75.6% of patients developed state of mental maladjustment of varying degree. In 47,1% of cases of mental disorders place in the form of psychogenic and somatogenically caused disorders of prenosological level. Among clinically executed forms predominated depressive disorder spectrum (nozogennye reaction and state). Shows the clinical and psychopathological features of these disorders and the need for complex therapy in cardiological clinic
-
 Роль комплексных лучевых методов в диагностике острого аппендицита у детей
Роль комплексных лучевых методов в диагностике острого аппендицита у детей
Prospects for the development of medicineОстрый аппендицит (ОА) представляет собой одно из наиболее распространённых заболеваний в ургентной абдоминальной хирургии. Поэтому в практической работе любой болевой синдром в нижней части живота справа предположительно расценивается в первую очередь как острый аппендицит. Однако, несмотря на достигнутые успехи в современной хирургии, на практике сохраняется большое количество патологических состояний, при которых своевременная диагностика острого аппендицита продолжает оставаться актуальной проблемой.
-
 Заболевания верхних дыхательных путей широко распространенны среди детского населения, которые наносят вред детскому организму. Инфекции дыхательных путей представляют собой одну из самых главных причин заболеваний в детском возрасте; около 70% этих инфекций поражает верхние дыхательные пути. Одним из наиболее частых клинических синдромов, встречающихся при ОРИ у детей, является острый ларинготрахеит. Актуальность проблемы острого ларинготрахеита обусловлена его высокой распространенностью, развитием бактериальных осложнений, наступлением летального исхода, склонностью к рецидивированию.
Заболевания верхних дыхательных путей широко распространенны среди детского населения, которые наносят вред детскому организму. Инфекции дыхательных путей представляют собой одну из самых главных причин заболеваний в детском возрасте; около 70% этих инфекций поражает верхние дыхательные пути. Одним из наиболее частых клинических синдромов, встречающихся при ОРИ у детей, является острый ларинготрахеит. Актуальность проблемы острого ларинготрахеита обусловлена его высокой распространенностью, развитием бактериальных осложнений, наступлением летального исхода, склонностью к рецидивированию. -
 During pregnancy, jaundice syndrome can develop as a complication of pregnancy, as well as in infectious and other pathological conditions. Timely establishment of the correct diagnosis in the development of jaundice in pregnant women is extremely important, since the management of pregnant women with viral hepatitis and women with jaundice due to pregnancy pathologies has significant differences. The development of jaundice in pregnancy can lead to such pathological conditions as indomitable vomiting of pregnant women, cholestatic hepatosis of pregnant women. The most important and difficult is the differential diagnosis of acute fatty hepatosis of pregnant women. Acute fatty liver of pregnancy is a rare occurring pathology of pregnancy: one case of acute fatty hepatosis of pregnant women occurs in 10,000-13,000 births. Consequently, in most maternity hospitals with the number of births of 3000-5000 per year, doctors theoretically have the opportunity to observe such a pathology of pregnant women once every three to four years [1,2]. As a rule, patients with AFGB are admitted to the infectious diseases hospital with suspicion of viral hepatitis, so the differential diagnosis is first of all, it is carried out with acute viral hepatitis (AVH) of various etiologies.
During pregnancy, jaundice syndrome can develop as a complication of pregnancy, as well as in infectious and other pathological conditions. Timely establishment of the correct diagnosis in the development of jaundice in pregnant women is extremely important, since the management of pregnant women with viral hepatitis and women with jaundice due to pregnancy pathologies has significant differences. The development of jaundice in pregnancy can lead to such pathological conditions as indomitable vomiting of pregnant women, cholestatic hepatosis of pregnant women. The most important and difficult is the differential diagnosis of acute fatty hepatosis of pregnant women. Acute fatty liver of pregnancy is a rare occurring pathology of pregnancy: one case of acute fatty hepatosis of pregnant women occurs in 10,000-13,000 births. Consequently, in most maternity hospitals with the number of births of 3000-5000 per year, doctors theoretically have the opportunity to observe such a pathology of pregnant women once every three to four years [1,2]. As a rule, patients with AFGB are admitted to the infectious diseases hospital with suspicion of viral hepatitis, so the differential diagnosis is first of all, it is carried out with acute viral hepatitis (AVH) of various etiologies. -
 Комплексная ультразвуковая диагностика острого аппендицита у детей
Комплексная ультразвуковая диагностика острого аппендицита у детей
Prospects for the development of medicineОстрый аппендицит является самым распространенным заболеванием, требующим проведения экстренного хирургического вмешательства. Встречаемость острого аппендицита составляет от 3 до 6 на 1000 детей. У детей острый аппендицит развивается быстрее, а деструктивные изменения в отростке, приводящие к аппендикулярному перитониту, возникают значительно чаще, чем у взрослых. Учитывая высокий процент необоснованных аппендэктомий в сомнительных случаях нами в стандарт диагностики острого аппендицита включено ультразвуковое исследование (УЗИ) червеобразного отростка.
-
 Комплексная лучевая диагностика острого аппендицита и его осложнений у детей
Комплексная лучевая диагностика острого аппендицита и его осложнений у детей
Scientific works of gifted youth and medicine of the XXI centuryОстрый аппендицит (ОА) представляет собой одно из наиболее распространённых заболеваний в ургентной абдоминальной хирургии. Поэтому в практической работе любой болевой синдром в нижней части живота справа предположительно расценивается в первую очередь как острый аппендицит. Однако, несмотря на достигнутые успехи в современной хирургии, на практике сохраняется большое количество патологических состояний, при которых своевременная диагностика острого аппендицита продолжает оставаться актуальной проблемой.
-

Острый аппендицит (ОА) - одно из самых распространенных хирургических заболеваний органов брюшной полости. Преимущественно им болеют в возрасте от 15 до 40 лет, что по новой возрастной классификации ВОЗ относят к молодому возрасту (от 25 до 44 лет), 44—60 лет — это средний возраст, 60—75 лет — пожилой возраст, 75—90 лет — это старческий возраст, а после 90 — это долгожители. Другими словами, ОА - заболевание людей молодого работоспособного возраста, что имеет свою практическую значимость. Внедрение в клиническую практику современных методов обследования позволило улучшить диагностику ОА и значительно оптимизировать результаты его лечения, но в старших возрастных группах повсеместного качественного улучшения диагностики не произошло, причем это касается как гиподиагностики, так и гипердиагностики.
-
 Features of diagnostics and differentiation of torsion and necrosis of the greater oil strand with acute cholecystitis (case report)
Features of diagnostics and differentiation of torsion and necrosis of the greater oil strand with acute cholecystitis (case report)
Modern trends in the development of science in the age of digitalizationTorsion and necrosis of the omentum strand is a casuistic disease and occurs in 0.06% – 0.14% of all urgent surgical pathologies in the abdominal organs. Taking into account the rare occurrence and the absence of a characteristic symptoms complex in the torsion of the omentum strand the preoperative diagnosis is correctly established in single cases. The etiology of the development of this pathology remains amystery in modern medicine and attracts more interest in itself due to the difficulty in diagnosis namely in the preoperative period. There are predisposing factors (adhesions in the abdominal cavity, ventral hernia, obesity, chronic inflammation of the abdominal organs) and producing factors (physical activity, eating a large amount of food, a sharp increase in intra-abdominal pressure or sudden contraction of the muscles of the anterior abdominal wall). Most often, the clinic of torsion of the omentum strand simulates such abdominal pathologies as acute appendicitis, acute intestinal obstruction of adhesive etiology, acute cholecystitis. Over the past decade, minimally
invasive surgery has become widespread, in particular laparoscopic surgery, as a
multi-port and single-port. The article highlights the difficulties of preoperative
diagnostics, the role of laparoscopy in differential diagnostics and the features of the
clinical course of torsion and necrosis of the fatty structures of the abdominal cavity -
 Комплексная эхография в диагностике острого аппендицита у детей
Комплексная эхография в диагностике острого аппендицита у детей
Scientific works of gifted youth and medicine of the XXI centuryОстрый аппендицит является самым распространенным заболеванием требующим проведения экстренного хирургического вмешательства. Встречаемость острого аппендицита составляет от 3 до 6 на I 000 детей. У детей острый аппендицит развивается быстрее, а деструктивные изменения в отростке, приводящие к аппендикулярному перитониту, возникают значительно чаще, чем у взрослых. Учитывая высокий процент необоснованных аппендэктомий в сомнительных случаях нами в стандарт диагностики острого аппендицита включено ультразвуковое исследование (УЗИ) червеобразного отростка.
-
 Definition. Acute bronchiolitis (J 21) is an acute infectious (mainly viral etiology) inflammatory disease of the lower respiratory tract, characterized by inflammation, edema and necrosis of epithelial cells, as well as increased mucus formation in the bronchioles, resulting in violation of air patency in the respiratory tract [2,13,21]. Clinically, the disease is characterized by an abundance of diffuse small moist and crepitant rales, an obsessive cough, usually marked shortness of breath and respiratory failure.
Definition. Acute bronchiolitis (J 21) is an acute infectious (mainly viral etiology) inflammatory disease of the lower respiratory tract, characterized by inflammation, edema and necrosis of epithelial cells, as well as increased mucus formation in the bronchioles, resulting in violation of air patency in the respiratory tract [2,13,21]. Clinically, the disease is characterized by an abundance of diffuse small moist and crepitant rales, an obsessive cough, usually marked shortness of breath and respiratory failure. -
 Комплексная лучевая диагностика острого аппендицита и его осложнений у детей
Комплексная лучевая диагностика острого аппендицита и его осложнений у детей
Scientific works of gifted youth and medicine of the XXI centuryОстрый аппендицит (ОА) представляет собой одно из наиболее распространённых заболеваний в ургентной абдоминальной хирургии. Поэтому в практической работе любой болевой синдром в нижней части живота справа предположительно расценивается в первую очередь как острый аппендицит. Однако, несмотря на достигнутые успехи в современной хирургии, на практике сохраняется большое количество патологических состояний, при которых своевременная диагностика острого аппендицита продолжает оставаться актуальной проблемой.