Library search
Search Results
-
 The current stage of development of the digital economy (DE) in Uzbekistan is characterized by a period of formation and high rates of development. Taking into account the adopted legislative and regulatory framework for the development of the DE and the comprehensive program for the development of the National Information and Communication System of the Republic, signifi cant results have been achieved. The analysis of the development indicators of the DE shows an increase in indicators, at the same time, the republic is not included in the list of countries actively developing the DE. Today, the banking system of Uzbekistan is actively introducing modern innovative ICT into activities, which is of great importance for the development of digitalization of banking activities. In the activity of the main division of the postal service of Uzbekistan represented by JSC "Uzbekistan Post" in recent years, there has been a deterioration in the main indicators. The assessment of the rating of the introduction of modern ICT at the enterprises of the republic, as well as numerous scientifi c studies carried out, showed that there are a number of problems. Despite the successes in the development of the republic’s DE, enterprises and organizations are noticeably lagging behind in the fi eld of introducing digital technologies into their activities. In particular, there are all the prerequisites and conditions for the formation and eff ective functioning of the basic institutions of the DE, but at the same time there are signifi cant barriers that hinder the further development of its institutional structure. To improve the situation, it is necessary to develop a comprehensive strategy for the digitalization of enterprises, focusing on the training of highly qualifi ed professional personnel for the modern IT market, innovative development and accelerated technological advancement.
The current stage of development of the digital economy (DE) in Uzbekistan is characterized by a period of formation and high rates of development. Taking into account the adopted legislative and regulatory framework for the development of the DE and the comprehensive program for the development of the National Information and Communication System of the Republic, signifi cant results have been achieved. The analysis of the development indicators of the DE shows an increase in indicators, at the same time, the republic is not included in the list of countries actively developing the DE. Today, the banking system of Uzbekistan is actively introducing modern innovative ICT into activities, which is of great importance for the development of digitalization of banking activities. In the activity of the main division of the postal service of Uzbekistan represented by JSC "Uzbekistan Post" in recent years, there has been a deterioration in the main indicators. The assessment of the rating of the introduction of modern ICT at the enterprises of the republic, as well as numerous scientifi c studies carried out, showed that there are a number of problems. Despite the successes in the development of the republic’s DE, enterprises and organizations are noticeably lagging behind in the fi eld of introducing digital technologies into their activities. In particular, there are all the prerequisites and conditions for the formation and eff ective functioning of the basic institutions of the DE, but at the same time there are signifi cant barriers that hinder the further development of its institutional structure. To improve the situation, it is necessary to develop a comprehensive strategy for the digitalization of enterprises, focusing on the training of highly qualifi ed professional personnel for the modern IT market, innovative development and accelerated technological advancement. -
 This article discusses the origins and features of the problems of the modern economic system. In a historical sight, the economic indicators of the pre-crisis and post-crisis periods are compared, the problems associated with an increase in the share of the stock market relative to the real sector of the economy, its causes and consequences are revealed.
This article discusses the origins and features of the problems of the modern economic system. In a historical sight, the economic indicators of the pre-crisis and post-crisis periods are compared, the problems associated with an increase in the share of the stock market relative to the real sector of the economy, its causes and consequences are revealed. -
 The article considers the draft concept "Digital Uzbekistan 2030" and describes the basic directions of digital development of Uzbekistan. The author examines the technological and sectoral models of digitalization, proposes a conceptual approach to the virtualization of the activities of enterprises in Uzbekistan based on the model of "digital twins".
The article considers the draft concept "Digital Uzbekistan 2030" and describes the basic directions of digital development of Uzbekistan. The author examines the technological and sectoral models of digitalization, proposes a conceptual approach to the virtualization of the activities of enterprises in Uzbekistan based on the model of "digital twins". -
Post-Traumatic Defects And Face Deformations: Features Of Diagnostics And Treatment
The American Journal of Medical Sciences and Pharmaceutical ResearchThe high growth of injuries, the absence in the country of a unified approach to the treatment of victims with pathology of the bones of the face and skull leads to a sharp increase in the number of patients with post-traumatic deformities, defects, often to their disability and death. This problem has recently acquired the greatest importance in connection with the increase in the number of victims in areas of natural disasters and road traffic accidents. Severe multiple fractures of the bones of the middle zone of the facial skeleton, accompanied by craniocerebral trauma of varying degrees, bleeding and liquorrhea, are often outwardly unnoticeable, since they are hidden by pronounced edema, hemorrhages in soft tissues, and can only be determined with a targeted specialized examination. These types of examinations and the provision of specialized medical care are possible only in multidisciplinary centers. Therefore, these types of injuries are not always diagnosed in a timely manner, especially in severely injured with the presence of pronounced injuries of other localizations.
-
Comparative Characteristics Of Rheological Properties Of Blood In Combined Face Injuries Before And After Treatment
The American Journal of Medical Sciences and Pharmaceutical ResearchFractures are one of the most common components in multiple and associated injuries. Fractures of the lower jaw are observed in 76%, of the upper jaw in 24%, a fracture of the zygomatic-orbital complex in 12%. The actual problem of modern traumatology is the violation of reparative osteogenesis with injuries combined with facial trauma. The duration of the consolidation of fractures is determined by the degree of microcirculation disorders in the fracture zone, changes in cellular and coagulation hemostasis and mineral metabolism. In this connection, increasing the effectiveness of treatment of fractures of the bones of the face on the basis of early diagnosis of vascular and hemostasiological changes is of great importance for practical health care.
-
Purulent-Necrotic Diseases Of The Face: Aspects Of Diagnostics And Treatment
The American Journal of Medical Sciences and Pharmaceutical ResearchThe problem of treatment of pyoinflammatory diseases (PID) of the face and neck is relevant for both dentists of polyclinics and maxillofacial surgeons in hospitals. About 50% of those in maxillofacial hospitals, and about 20% of those who seek help from a dentist and a surgeon of polyclinics, are patients with inflammatory diseases of the maxillofacial region (MFO), among them - 60-80% of patients with abscesses and phlegmons, the frequency of which has increased by 1.5–2.0 times over the past decade. There has been a steady growth of atypical and severely flowing progressive phlegmon, spreading simultaneously in several cellular spaces, with the development of such formidable complications as sepsis, contact mediastinitis, and thrombosis of the cavernous sinus of the dura mater. Low-symptom “erased” forms of phlegmon are found among 13.4–22% of patients, are characterized by a long course and are difficult to diagnose, which contributes to late hospitalization and untimely treatment started. Microbial etiology of HVZ CLO is due to the localization of the primary process (connection with the oral cavity, teeth).
-
Overview Of Comprehensive Treatment Of Acute Purulent-Inflammatory Diseases Of The Face And Neck
The American Journal of Medical Sciences and Pharmaceutical ResearchThe aim of the work is to systematize the data of special literature for the clearest definition of the directions of studying the modern approach to the diagnosis, prognosis and treatment of pyoinflammatory processes in the maxillofacial region and neck. As a result of the analysis of the data of special literature, it becomes obvious that in recent decades the idea of the etiology and pathogenesis of pyoinflammatory processes in the maxillofacial region and neck has changed, which determines the need for further search for new informative methods of diagnosis, prognosis, as well as the most effective methods of treatment and prevention of complications for this pathology.
-
 Hozirgi kunda mamlakatimizni isloh etish va modernizatsiya qilish hamma sohalarda, shuningdek sog’likni saqlash tizimida ham amalga oshirilmoqda. Buning asosiy inaqsadi, aholini sog’Iigini mustahkamlash, tibbiy yordam sifatini yanada oshirish, sog’likni saqlashni birlamchi tizimini mustahkamlash, profilaktika yonalishini rivojlantirish, aholini talabini ilmiy asoslangan yuqori texnologik tibbiy yordam bi lan qondirishdir.
Hozirgi kunda mamlakatimizni isloh etish va modernizatsiya qilish hamma sohalarda, shuningdek sog’likni saqlash tizimida ham amalga oshirilmoqda. Buning asosiy inaqsadi, aholini sog’Iigini mustahkamlash, tibbiy yordam sifatini yanada oshirish, sog’likni saqlashni birlamchi tizimini mustahkamlash, profilaktika yonalishini rivojlantirish, aholini talabini ilmiy asoslangan yuqori texnologik tibbiy yordam bi lan qondirishdir. -
 ISSUES OF DEVELOPING AN EFFECTIVE SYSTEM OF COMBATING TERRORISM AND RELIGIOUS EXTREMISMIn this article, in today's globalization and at a time when the transformation of international and regional conflicts continues, the issues of effective fight against terrorism and religious extremism are scientifically covered.
ISSUES OF DEVELOPING AN EFFECTIVE SYSTEM OF COMBATING TERRORISM AND RELIGIOUS EXTREMISMIn this article, in today's globalization and at a time when the transformation of international and regional conflicts continues, the issues of effective fight against terrorism and religious extremism are scientifically covered.
Modern Science and Research -
 Юз суякларининг қўшма жароҳатларида бурун ёндош бўшлиқлари жароҳатлари бўлган беморларни текширув натижалари
Юз суякларининг қўшма жароҳатларида бурун ёндош бўшлиқлари жароҳатлари бўлган беморларни текширув натижалари
Actual problems of dentistry and maxillofacial surgery 4Юз-жағ соҳаси қўшма жароҳатларида калла суяклари, бурун ва бурун ёндош бўшлиқларининг биргаликда шикастланишлари туфайли шифохоналар
жонлантириш бўлимларида йилдан йилга беморлар сони ошиб бораётганлиги амалиётда кузатилмоқда. -
 Бурун ёндош бўшлиқлари жароҳатларини юз суякларининг қўшма жароҳатларида ташхислаш
Бурун ёндош бўшлиқлари жароҳатларини юз суякларининг қўшма жароҳатларида ташхислаш
Actual problems of dentistry and maxillofacial surgery 4Юз суякларининг қўшма жароҳатлари бор беморларда бурун ва бурун ёндош бўлиқлари жароҳатларини эрта ташхислаш.
-
 Оценка эффективности лечения сочетанных травм с повреждением верхнечелюстной пазухи
Оценка эффективности лечения сочетанных травм с повреждением верхнечелюстной пазухи
Days of young scientistsУсовершенствование тактики оказания лечебно-диагностической помощи при сочетанных травмах верхнечелюстной пазухи.
-
STATE OF THE DENTOALVEOLAR SYSTEM IN PATIENTS WITH POSTTRAUMATIC NASAL DEFORMITIES
European International Journal of Multidisciplinary Research and Management StudiesIn modern conditions of society development, improving the quality of medical care is of extremely important social significance. Scientific and technological progress and the totality of modern social relations impose increasingly high professional, moral, ethical and legal requirements to specialists in the field of health care [1,2,5].
-
ORBITAL WALL FRACTURE IN COMBINED INJURIES OF BONES OF THE FACIAL SKELETON
The American Journal of Medical Sciences and Pharmaceutical ResearchCombined injury of the maxillofacial region remains one of the topical problems of maxillofacial traumatology. Combined trauma to the maxillofacial region requires joint medical care by several specialists. Trauma of the upper and middle zones of the face is often accompanied by trauma of the eye socket, paranasal sinuses. They are difficult to diagnose, in case of untimely diagnosis and rendered assistance lead to secondary defects and deformities. Damage to the walls of the orbit, leads to scarring changes in the fiber of the eye socket, eye muscles, persistent diplopia, ocular nerve impingement, persistent eye asymmetry, decreased or loss of vision is the cause of frequent disability.
-
 Improvement of diagnosis and treatment of patients with combined trauma of facial bone
Improvement of diagnosis and treatment of patients with combined trauma of facial bone
Catalog of abstractsTopicality and demand of the subject of dissertation. In the world lat days chanchcd structures of trauma, increase the number of heavy combined traumas, which resulting in more heavy nature of simultaneous injuries of three , four or more anatomical regions, which creates difficulties in determining of the order of care and surgical tactics in patients with combined traumas of the facial skeleton bones (CTFSB). The syndrome of mutual burdening injuries of various anatomical regions, variety, hcavity and speed of the development of pathological process did difficulty of diagnosis of the CTFSB. Complexity of the clinical picture, features of the progress of post-traumatic shock, the development of traumatic disease cause difficulties which arise in the course of examination of patients and put tasks to the experts to find new ways of developing diagnostic algorithms and early surgical treatment of the CTFSB.
Frequency of CTFSB ranges from 34,8 to 63,3%. Fractures of orbit has been observed with an extremely high frequency (98%) in CTFSB, injury of the orbit is accompanied by damage of the eyeball and its subsidiary bodies has been observed in 66 % of eases. Consequences of eye injuries arc becoming the leading cause of disability and in 50% of eases could cause permanent loss of vision. By reason of death combined trauma take the third part after coronary heart diseases. Frequency of disfiguring defects and deformities of face occurs in 12 and 57%, disability in CTFSB reaches up to 23%. CTFSB, combined with TBI, causes up to 60% of deaths.
The causes of unsufficient results is non-availability of a diagnostic algorithm, which includes the most informative research methods, determining the order of interaction and priority of work of doctors of various specialties in CTFSB.
In some eases, requires specified an indications, character, scope, sequence and timing of surgical interventions, depending of the objective assessment of heaviness of injuries to various anatomical regions, prognosis criteria, the nature and heaviness of life-threatening consequences of combined trauma. The research work earned out within the framework of the achievement of the set by the Decree of the President of Republic of Uzbekistan “About measures on the further deepening reform the health care system” November 28, 2011, № PD-1652, maintenance of high-quality medical aid to the population under modem requirements and standards.In this regard the need for the development of algorithms of diagnosis and early methods of surgical treatment of patients with CTFSB constitute one of the important criteria demand the theme of dissertation.
Purpose of research is improvement of the diagnostic tactics and therapeutic interventions in patients with acute combined injuries of the facial bones according to the severity and location of the injury.
Scientific novelty of disscrtational research consists in the following: revealed the structure and features provide consistent care to patients with combined injuries in Republic of Uzbekistan;
The sequence of diagnostic and therapeutic measures, depending on the patient's general condition with CTFSB first determined by using created CT program "ADIL
developed innovative methods for early reduction and fixation of bone fragments in CTFSB;
identified endogenous factors, affecting on the wound process, disclosed the mechanisms of post-traumatic complications in CTFSB;
proved, that at 2 - 3rd days after the injury occurs the depression of cell and humoral immunity in the blood. Increases the level of proinflammatory cytokines, reduced the level of anti-inflammatory cytokine (in 2,8 at patients with heavy commonl condition. Increased levels of pro - and reducing anti - inflammatory cytokines is a poor prognostic factor in the development of inflammatory complications (bone wound suppuration, osteomyelitis of the jaw bones, soft tissue abscess);
patients with CTFSB at 2 - 3rd days after the injury occurs the depression of the content of protein and micronutrients (calcium, potassium and phosphorus) in the blood, which is a prognostic factor of the development of complications;
a scheme was developed for integrated medical correction of endogenous factors affecting on the development of posttraumatic complications;
1. CTFSB in 100% of cases combined with TBI, in 27.7 % with injuries of skeleton and internal injuries. In the diagnosis and treatment of patients with CTFSB should participate resuscitator, maxillofacial surgeon, neurosurgeon, ophthalmologist, and otolaryngologist. Primary debridement of wounds, reduction and fixation of bone fragments in patients in compensated state should be done within 3 hours after injury, while at subcompensated state - during the first day, and at the decompensated state - within 3 days.
2. With the CT program "ADIL" can determine the overall condition of patients in a short time. The most informative diagnostic criteria arc the general condition of patients, level of consciousness, hemodynamic stability, shock index and temperature gradient. The severity of the general condition of patients is directly dependent on the localization of the fracture of the facial bones. Multiple fractures of the upper and middle areas of the face arc the most serious injury in patients.
3. Patients with CTFSB in compensated and subcompensated state emergency surgical aid and diagnostic procedures should be performed in full volume (maxillofacial surgery, traumatology, neurosurgery, surgery, ophthalmology and otorhinolaryngologist), including the reduction and fixation of bone fragments in the first day. To patients with CTFSB in state decompensated should be performed at least diagnostic procedures, limiting the amount of emergency surgery. Reduction and fixation of bone fragments should be done after the restoration of function of vital organs and systems.
4. The method of choice for the treatment of depressed large bone fragments of facial bones is a titanium distractor, the use of which gives a good clinical and functional outcome.
5. When depressed fracture of the zygomatic arch application of the developed device will allow us to produce reduction and fixation of bone fragments in the early stages (within one day) with a good cosmetic result.
6. At patients with CTFSB in posttraumatic period (7- 14th day.) there arc a deep depression of CD3, CD4 cell composition, humoral factors and secretory immune system, increased necrosis factor CD95, increasing the levels of proin-flammatory (IL-6 ) and a decrease - anti- inflammatory (IL -10) cytokines. On 9-10th day reduced total protein, calcium, potassium and phosphorus in the blood .
7. Reduction of cellular and humoral immunity, increased proinflammatory cytokine and tumor necrosis factor, reducing the anti-inflammatory cytokine , the protein concentration in the blood, calcium, potassium and phosphorus arc predictors of complications.
8. Application of complex drug therapy within the 1-3 days after the injury with the inclusion of immune ( immunomoduline, ribomunil ), enzyme ( Voben-zym ) drugs osteoplastic materials allows to correct the violation of homeostasis, also used to prevent complications. -
 Study of foaming in clay suspensions depending on the content and nature of the surfactant
Study of foaming in clay suspensions depending on the content and nature of the surfactant
Central Asian Food Engineering And TechnologyThe article presents the results of an experiment to study the effect of surfactant concentration and type on foam formation in clay suspensions. As a result of the study, it was found that the addition of surfactants to the system leads to an increase in the volume of foam, and the most significant effect is observed when using surfactants of the type OP-10. With an increase in the concentration of surfactants to a specific value (0.3%), a sharp increase in the height of the foam is observed; however, a further increase in the concentration does not have a significant effect on the
amount of the formed foam. The study also showed that the height of the foam in the system with surfactant type OP-10 is higher than in the system with surfactant type GKJ-11, which indicates greater foam adsorption at the liquid-air interface. The study of the surface tension of surfactant solutions showed that the surfactant type OP-10 has more significant properties of the surfactant than the surfactant type GKJ-11. These results may be useful to improve the foaming in slurry drilling fluids using various types and concentrations of surfactants. -
 The results of the study of hydraulic pressure in the roll squeezing of wet materials are given. Mathematical models of hydraulic pressure distribution in the squeezing zone are developed. It is revealed that the hydraulic pressure in the compression zone increases from zero at the initial contact point to a maximum at a point lying on the line of centers. The distribution patterns of hydraulic pressure in the strain restoration zone depend on the length of its part, where the fluid flows from the wet material into the roll coating.
The results of the study of hydraulic pressure in the roll squeezing of wet materials are given. Mathematical models of hydraulic pressure distribution in the squeezing zone are developed. It is revealed that the hydraulic pressure in the compression zone increases from zero at the initial contact point to a maximum at a point lying on the line of centers. The distribution patterns of hydraulic pressure in the strain restoration zone depend on the length of its part, where the fluid flows from the wet material into the roll coating. -
 SHAMOL ELEKTR STANSIYALARINING CHIQISH KUCHLANISH PARAMETRLARINI ROSTLASH USULLARINI TADQIQ ETISHushbu ishda shamol elektr stansiyalarida ikki o‘qi bo‘yicha qo‘zg‘atiladigan sinxron generatorlarni qo‘llash masalasi ko‘rilgan va bunday generatorlarning afzalliklari keltirilgan.
SHAMOL ELEKTR STANSIYALARINING CHIQISH KUCHLANISH PARAMETRLARINI ROSTLASH USULLARINI TADQIQ ETISHushbu ishda shamol elektr stansiyalarida ikki o‘qi bo‘yicha qo‘zg‘atiladigan sinxron generatorlarni qo‘llash masalasi ko‘rilgan va bunday generatorlarning afzalliklari keltirilgan.
Modern Science and Research -
 SHAMOL ELEKTR STANSIYALARIDA IKKI O‘QI BO‘YICHA QO‘ZGʻATILADIGAN SINXRON GENERATORLARNI ISHLATISHUshbu ishda shamol elektr stansiyalarida ikki o‘qi bo‘yicha qo‘zg‘atiladigan sinxron generatorlarni qo‘llash masalasi ko‘rilgan va bunday generatorlarning afzalliklari keltirilgan
SHAMOL ELEKTR STANSIYALARIDA IKKI O‘QI BO‘YICHA QO‘ZGʻATILADIGAN SINXRON GENERATORLARNI ISHLATISHUshbu ishda shamol elektr stansiyalarida ikki o‘qi bo‘yicha qo‘zg‘atiladigan sinxron generatorlarni qo‘llash masalasi ko‘rilgan va bunday generatorlarning afzalliklari keltirilgan
Modern Science and Research -
 Tactics of treatment of acute abscess in children early ageThe article deals with an acute abscess (OP) in infancy and infancy, which occurs much more fre-quently than in other age groups, the children of the first months of life constitute more than 50%. When pu-rulent-inflammatory diseases of the frequency of the OP in infants is 1.9 times higher than in children older than 1 year and the largest number (42.5%) are in the first 3 months of life Other researchers have noted that the first year of the child OP life is observed in 60% of cases among children of all age groups
Tactics of treatment of acute abscess in children early ageThe article deals with an acute abscess (OP) in infancy and infancy, which occurs much more fre-quently than in other age groups, the children of the first months of life constitute more than 50%. When pu-rulent-inflammatory diseases of the frequency of the OP in infants is 1.9 times higher than in children older than 1 year and the largest number (42.5%) are in the first 3 months of life Other researchers have noted that the first year of the child OP life is observed in 60% of cases among children of all age groups
Journal problems of biology and medicine -
 Innovative methods of treatment of the combined injuries of bones of the facial skeleton on the basis of algorithmization of activity of the doctorThe developed algorithm of the organization of the stomatologic help to patients with the combined in-jury of bones of a facial skeleton consists of three blocks of the actions rendered in a reception, the medical and diagnostic actions and events held in the first 3 hours by experts. Also it is offered to establish algorith-mic dependences of a condition of patients with last diseases of particular persons, in similar situations, for this purpose programs have to be archived and be stored on the server. If necessary the computer on a net-work in the automatic mode can send to this server inquiry on each patient. Then search regarding is carried out, whether this person at inspection participated in the same quality earlier, and all information will go on a network to the stomatologist's computer. The condition of the examined patients recorded in the above-named archives will be considered in an automatic order.
Innovative methods of treatment of the combined injuries of bones of the facial skeleton on the basis of algorithmization of activity of the doctorThe developed algorithm of the organization of the stomatologic help to patients with the combined in-jury of bones of a facial skeleton consists of three blocks of the actions rendered in a reception, the medical and diagnostic actions and events held in the first 3 hours by experts. Also it is offered to establish algorith-mic dependences of a condition of patients with last diseases of particular persons, in similar situations, for this purpose programs have to be archived and be stored on the server. If necessary the computer on a net-work in the automatic mode can send to this server inquiry on each patient. Then search regarding is carried out, whether this person at inspection participated in the same quality earlier, and all information will go on a network to the stomatologist's computer. The condition of the examined patients recorded in the above-named archives will be considered in an automatic order.
Journal problems of biology and medicine -
 In the recent year the number of injuries with maxillofacial trauma has significantly increased in all countries of the world is. Despite the continuous improvement of the treatment methods of jaw fractures, the periods of immobilization and temporary disability are not reduced, and the incidence of inflammatory complications remains high, which significantly worsens the outcome of trauma. At the same time, little attention is paid to nutritional insufficiency of patients, which is the cause of decreased immunity, a weakening of the body’s defenses, an increased risk of complications, prolonged healing of wounds and bones and other changes. This review article examines the studies conducted on the nutrition of patients with the jaw fractures and gives brief information about main points of this researches.
In the recent year the number of injuries with maxillofacial trauma has significantly increased in all countries of the world is. Despite the continuous improvement of the treatment methods of jaw fractures, the periods of immobilization and temporary disability are not reduced, and the incidence of inflammatory complications remains high, which significantly worsens the outcome of trauma. At the same time, little attention is paid to nutritional insufficiency of patients, which is the cause of decreased immunity, a weakening of the body’s defenses, an increased risk of complications, prolonged healing of wounds and bones and other changes. This review article examines the studies conducted on the nutrition of patients with the jaw fractures and gives brief information about main points of this researches. -
 COMPARATIVE ANALYSIS OF THE FREQUENCY OF RS1801133 POLYMORPHISM OF THE MTHFR GENE IN THE GROUP OF PATIENTS WITH POSTCOVID COMPLICATIONS OF MAXILLOFACIAL AREAIn the article of genetic studies of patients with post-covid maxillofacial complications. The condition after COVID-19 is considered a life-threatening disease, ranging from mild symptoms to serious complications. Candidiasis is the most common type of superficial purulent infection. The Candida species is a frequent inhabitant of the oral mucosa, but its growth is inhibited by other organisms in the body, which prevents any pathological change in the mucous membrane of this fungus. Candida albicans is the most common yeast, followed by Candida glabrata, Candida krusei, Candida tropicalis and Candida stellatoidea. According to this systematic review, 57 cases of oral candidiasis and one case of retinitis candidiasis were reported in patients undergoing treatment for COVID-19. Single-cell RNA-seq analysis of angiotensin-converting enzyme II (ACE2) expression and serologic examination of samples indicates that ACE2 may be the cellular receptor for SARS-CoV-2, suggesting that ACE2-expressing cells are likely to be the main target cell type that vulnerable to SARS-CoV-2 infection. As a rule, there is a high expression of ACE2 r on the epithelial cells of the oral mucosa, enrichment is enriched in epithelial cells of the tongue. There were few reports prior to this study.
COMPARATIVE ANALYSIS OF THE FREQUENCY OF RS1801133 POLYMORPHISM OF THE MTHFR GENE IN THE GROUP OF PATIENTS WITH POSTCOVID COMPLICATIONS OF MAXILLOFACIAL AREAIn the article of genetic studies of patients with post-covid maxillofacial complications. The condition after COVID-19 is considered a life-threatening disease, ranging from mild symptoms to serious complications. Candidiasis is the most common type of superficial purulent infection. The Candida species is a frequent inhabitant of the oral mucosa, but its growth is inhibited by other organisms in the body, which prevents any pathological change in the mucous membrane of this fungus. Candida albicans is the most common yeast, followed by Candida glabrata, Candida krusei, Candida tropicalis and Candida stellatoidea. According to this systematic review, 57 cases of oral candidiasis and one case of retinitis candidiasis were reported in patients undergoing treatment for COVID-19. Single-cell RNA-seq analysis of angiotensin-converting enzyme II (ACE2) expression and serologic examination of samples indicates that ACE2 may be the cellular receptor for SARS-CoV-2, suggesting that ACE2-expressing cells are likely to be the main target cell type that vulnerable to SARS-CoV-2 infection. As a rule, there is a high expression of ACE2 r on the epithelial cells of the oral mucosa, enrichment is enriched in epithelial cells of the tongue. There were few reports prior to this study.
The American Journal of Medical Sciences and Pharmaceutical Research -
 Modern aspects of diagnostic and planning of surgical treatment of zygomati- corbital fracturesThis article provides a summary of the literature data on the diagnosis and planning of surgical treatment of patients with fractures of the zygomatic-orbital complex. Despite the large number of works devoted to this topic, the literature data on the choice of diagnostic methods and planning of surgical treatment are rather fragmentary and not systematized, which in turn allows us to focus our activities and research on the development and modernization of diagnostic methods and surgical treatment of fractures of the zygomatic-orbital complex.
Modern aspects of diagnostic and planning of surgical treatment of zygomati- corbital fracturesThis article provides a summary of the literature data on the diagnosis and planning of surgical treatment of patients with fractures of the zygomatic-orbital complex. Despite the large number of works devoted to this topic, the literature data on the choice of diagnostic methods and planning of surgical treatment are rather fragmentary and not systematized, which in turn allows us to focus our activities and research on the development and modernization of diagnostic methods and surgical treatment of fractures of the zygomatic-orbital complex.
Doctor's Herald -
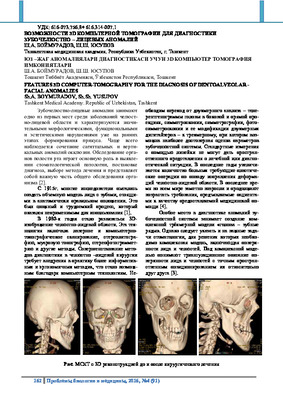 Features 3d computer-tomography for the diagnosis of dentoalveolar - facial anomaliesDental and maxillofacial anomalies occupy one of the first places among the diseases of the maxillofacial region and are characterized by significant morphological, functional and aesthetic disorders already in the early stages of bite formation. Most often there is a combination of sagittal and vertical anomalies of occlusion. Examination of the organs of the oral cavity plays a major role in identifying dental pathology, making a diagnosis, choosing a method of treatment and represents is an important part of the general examination of the body [2].
Features 3d computer-tomography for the diagnosis of dentoalveolar - facial anomaliesDental and maxillofacial anomalies occupy one of the first places among the diseases of the maxillofacial region and are characterized by significant morphological, functional and aesthetic disorders already in the early stages of bite formation. Most often there is a combination of sagittal and vertical anomalies of occlusion. Examination of the organs of the oral cavity plays a major role in identifying dental pathology, making a diagnosis, choosing a method of treatment and represents is an important part of the general examination of the body [2].
Journal problems of biology and medicine