Library search
Search Results
-
 The purpose of the work is to study the topographic anatomy and macroscopic structure of the gallbladder and biliary tract in newborns, children and adolescents. Material and research methods. The object of the study was 54 corpses of newborns, children and adolescents of both sexes up to 16 years old. with body weight from 3.0 kg to 55 kg, who died for reasons not related to pathology of the liver and bile ducts. Studied in detail the formation of the common bile duct, the options for its formation. Results, /\ge-related changes in the topography of the ducts concerned the length, diameter, depth, the number of branches and the severity of anastomoses between segmental branches and between the lobar ducts. The diameter of the common hepatic duct ranged from 1.1 mm to 5.0 mm, the right hepatic duct from 0.87 mm to 3.06 mm. and the left hepatic duct from 0.89 mm to 3.03 mm in different age groups. The length of the total hepatic duct is from 4.5 mm to 35.8 mm. When considering the angles of incidence between the common hepatic and left and right ducts varies. Conclusion. The results showed that in children of all age groups the formation of the common hepatic duct is variable; 2 to 5 intrahepatic ducts take part in its formation, while the number of ducts coming from the right lobe of the liver prevails.
The purpose of the work is to study the topographic anatomy and macroscopic structure of the gallbladder and biliary tract in newborns, children and adolescents. Material and research methods. The object of the study was 54 corpses of newborns, children and adolescents of both sexes up to 16 years old. with body weight from 3.0 kg to 55 kg, who died for reasons not related to pathology of the liver and bile ducts. Studied in detail the formation of the common bile duct, the options for its formation. Results, /\ge-related changes in the topography of the ducts concerned the length, diameter, depth, the number of branches and the severity of anastomoses between segmental branches and between the lobar ducts. The diameter of the common hepatic duct ranged from 1.1 mm to 5.0 mm, the right hepatic duct from 0.87 mm to 3.06 mm. and the left hepatic duct from 0.89 mm to 3.03 mm in different age groups. The length of the total hepatic duct is from 4.5 mm to 35.8 mm. When considering the angles of incidence between the common hepatic and left and right ducts varies. Conclusion. The results showed that in children of all age groups the formation of the common hepatic duct is variable; 2 to 5 intrahepatic ducts take part in its formation, while the number of ducts coming from the right lobe of the liver prevails. -
 Morphology of the intramural nervous apparatus of the common bile ductNeurohistological methods of investigation have been used to study the intramural nervous apparatus of the common bile duct wall. An abundance of nerve elements in the wall of the common bile duct is established. Nerve nodes, nerve cells and receptors are found. The main number of receptors is concentrated in the terminal section of the common bile duct, that is, at the site of opening the ampule of the faters papilla in the gut
Morphology of the intramural nervous apparatus of the common bile ductNeurohistological methods of investigation have been used to study the intramural nervous apparatus of the common bile duct wall. An abundance of nerve elements in the wall of the common bile duct is established. Nerve nodes, nerve cells and receptors are found. The main number of receptors is concentrated in the terminal section of the common bile duct, that is, at the site of opening the ampule of the faters papilla in the gut
Journal problems of biology and medicine -
Evaluation of the effectiveness of our chosen approach in the treatment of this
disease, which is confirmed by the results obtained – a low percentage of relapses of the disease, a
reduction in the need for additional treatment, a reduction in the duration of the patient’s stay in the
hospital, as well as the feasibility of early aspiration of purulent contents through the skin, preventing
spontaneous opening of the abscess with subsequent probing and washing of the tear ducts. -
A differentiated approach in the treatment of phlegmon of the lacrimal sac, taking into account
the etiopathogenesis of the disease and the presence of concomitant pathology, helps to reduce the recurrence of the disease, the need for additional treatment, as well as a decrease in the inpatient number of patients. -
 Diagnostic and surgical tactics of cholelithiasis diseases complicated by cholecystobiliary fistula (mirizzi syndrome type ii)
Diagnostic and surgical tactics of cholelithiasis diseases complicated by cholecystobiliary fistula (mirizzi syndrome type ii)
Doctor's HeraldThe article dedicated for issues of surgical correction of Mirrizzi'syndrome type 2. This is one of the difficult complication with forming of gallbladder-duct fistula, very often - with mechanical jaundice and purulent cholangitis. Authors had observed 63 patients with gallbladder-duct fistula and resulted to conclusion of complex treatment starting from endoscopy. At low efficacy of endoscopy authors admitted patients for open surgical operations urgently. One of the ways to operate is fistula plastic with remodeling of gallbladder duct and CBD drainaging through new wall-formed channel. Key words: CBD, mechanical jaundice, gallbladder-duct fistula, Mirrizzi syndrome, purulent cholangitis
-
 Факторный анализ ближайших и отдаленных результатов лечения «свежих» повреждений магистральных желчных путейПроанализированы результаты хирургического лечения 103 больных со «свежими» повреждениями МЖИ. Основной операцией при полном пересечении и иссечении ВЖП является ГепЕА по Ру, что выполнено 67 больным с хорошими отдаленными результатами в 97,0%. Восстановительная операция показана только при парциальном повреждении протока, формирование ББА при полном пересечении протока во всех случаях завершилась стриктурой. ГепДА также отрицательно сказалась на результатах лечения. Осложнения в ближайшем послеоперационном периоде были в 17,5%, в отдаленном - 33,9%. Повторные оперативные вмешательства выполнены 32,03% больным, летальность - 5.8%
Факторный анализ ближайших и отдаленных результатов лечения «свежих» повреждений магистральных желчных путейПроанализированы результаты хирургического лечения 103 больных со «свежими» повреждениями МЖИ. Основной операцией при полном пересечении и иссечении ВЖП является ГепЕА по Ру, что выполнено 67 больным с хорошими отдаленными результатами в 97,0%. Восстановительная операция показана только при парциальном повреждении протока, формирование ББА при полном пересечении протока во всех случаях завершилась стриктурой. ГепДА также отрицательно сказалась на результатах лечения. Осложнения в ближайшем послеоперационном периоде были в 17,5%, в отдаленном - 33,9%. Повторные оперативные вмешательства выполнены 32,03% больным, летальность - 5.8%
Doctor's Herald -
 Improvement of surgical treatment of intraoperative injuries of bile ductsThe results of surgical treatment of 131 patients with intraoperative bile ducts injuries have been analysed. The main operation in complete extrahepatic bile ducts transaction and excision is HepJA according to Roux that had been performed in 64 patients with a good follow – up result making 95,3%. Restorative operation is only indicated in partial injury of the duct. BBA formation in complete transaction of the duct in all cases resulted in stricture. HepDA also produced negative results of treatment. Complications in the near – by postoperative period made 20,3% and in the follow – up period 36,4%. Repeated operative interventions were performed in 33,9% of patients, lethal outcome made 5,8%.
Improvement of surgical treatment of intraoperative injuries of bile ductsThe results of surgical treatment of 131 patients with intraoperative bile ducts injuries have been analysed. The main operation in complete extrahepatic bile ducts transaction and excision is HepJA according to Roux that had been performed in 64 patients with a good follow – up result making 95,3%. Restorative operation is only indicated in partial injury of the duct. BBA formation in complete transaction of the duct in all cases resulted in stricture. HepDA also produced negative results of treatment. Complications in the near – by postoperative period made 20,3% and in the follow – up period 36,4%. Repeated operative interventions were performed in 33,9% of patients, lethal outcome made 5,8%.
Journal problems of biology and medicine -
 Анатомия и хирургия грудного лимфатического протокаВ статье приведены литературные данные по анатомии и хирургии грудного лимфатического протока и его значение теоритической и практической ветеринарии и медицины.
Анатомия и хирургия грудного лимфатического протокаВ статье приведены литературные данные по анатомии и хирургии грудного лимфатического протока и его значение теоритической и практической ветеринарии и медицины.
Prospects for the development of veterinary science and its role in ensuring food safety -
 The mucocele of the paranasal sinuses is a kind of retention saccular cyst of any one paranasal sinus, which is formed as a result of obliteration of the nasal excretory duct and the accumulation of mucous and hyaline secretion inside the sinus, as well as elements of desquamation of the epithelium [1, 3, 6]. Most often, the mucocele of the paranasal sinuses is localized in the frontal sinus (80%), then in the ethmoid labyrinth (15%) or on the border between them, which often leads to the penetration of the “cyst” into the orbit,calling exophthalmos, a fact that explains its frequent detection by ophthalmologists. Very rarely, the mucocele is localized in the sphenoid and maxillary sinuses (5%).
The mucocele of the paranasal sinuses is a kind of retention saccular cyst of any one paranasal sinus, which is formed as a result of obliteration of the nasal excretory duct and the accumulation of mucous and hyaline secretion inside the sinus, as well as elements of desquamation of the epithelium [1, 3, 6]. Most often, the mucocele of the paranasal sinuses is localized in the frontal sinus (80%), then in the ethmoid labyrinth (15%) or on the border between them, which often leads to the penetration of the “cyst” into the orbit,calling exophthalmos, a fact that explains its frequent detection by ophthalmologists. Very rarely, the mucocele is localized in the sphenoid and maxillary sinuses (5%). -
 This article presents the issues of surgical reconstruction of the larynx in injuries of the thyroid membrane. We use two types of thyrohyoidopexy in case of injuries of the thwoid membrane. In the first version of surgery. we perform in the early period after an open or closed injur,' of the thyroid membrane. The second version of the surgery is used in case of old closed injuries of the thyroid membrane, that is. when the persistent effects of this injury are stated as a scarry stenosis of the larynx with a defect in the front wall. In order to well mobilize the larynx, it is enough to cut only the sternothyroid muscles, and others use for better fixation of the anastomosis. In case of persistent effects of the old injuries of thyroid membrane, the method of choice can be the ability of the implantation of fragment of the body of the hyoid bone and the epiglottis into the cleft thyroid cartilage.
This article presents the issues of surgical reconstruction of the larynx in injuries of the thyroid membrane. We use two types of thyrohyoidopexy in case of injuries of the thwoid membrane. In the first version of surgery. we perform in the early period after an open or closed injur,' of the thyroid membrane. The second version of the surgery is used in case of old closed injuries of the thyroid membrane, that is. when the persistent effects of this injury are stated as a scarry stenosis of the larynx with a defect in the front wall. In order to well mobilize the larynx, it is enough to cut only the sternothyroid muscles, and others use for better fixation of the anastomosis. In case of persistent effects of the old injuries of thyroid membrane, the method of choice can be the ability of the implantation of fragment of the body of the hyoid bone and the epiglottis into the cleft thyroid cartilage. -
 Ўткир бош мия қон томир патологиялари ривожланишида коллатерал қон билан таъминланишининг ўзига хослигининг аҳамияти
Ўткир бош мия қон томир патологиялари ривожланишида коллатерал қон билан таъминланишининг ўзига хослигининг аҳамияти
NeurologyБош мия қон-томир касалликлари тиббиётда ва иж тимоий ҳаётда долзарб муаммолардан бири бўлиб келмоқда. Ер юзида ЖССТ берган маълумотга кўра ҳар йили 15 млн.дан ортиқ аҳоли инсульт ташхиси билан рўйҳатга олинади, шуларнинг ярмидан кўпида 1 йил давомида ўлим ҳодисаси кузатилади. Тирик қолганларнинг 80%дан ортиғида ногиронлик келиб чиқади (27,26,19). Дастлабки 1-йилда инсульт ўтказганларнинг 5-25% ида қайта инсульт кузатилади, кейинги 5 йилда эса 20-40% беморларда кузатилади ( 21,8.). Такрорий инсульт натижасида эса 95-100% беморлар ногирон бўлиб қолишади ва уларнинг 65-80% и бегоналар ёрдамига мухтож бўладилар. 70% касалларда эса психик бузилишлар кузатилади (28). РАМН(РТФА) берган маълумотларга кўра ишемик инсульт(ИИ) билан касалланган беморларнинг 84,5% и 55 ёшдан юқори бўлган беморлар, эркаклар орасида бу кўрсаткич 40-55 ёшда 30% ни, аёллар орасида эса 40-60 ёшда 46,2% ни ташкил этади (6). Охирги йилларда инсультнинг бундай ёшариши бу муаммони нг долзарблигини янада оширмоқда.
-
 Epidemiologic and morphologic characteristic of congenital obstruction of small intestine in newborn babiesMorphology of jejunum of experimental animals has identical structural changes with morphology of jejunum in newborn babies with congenital abnormalities of small intestine. Solving of the problems regarding malformations of small intestine in new born babies is actively needed to transfer to the aspect of preventive measures
Epidemiologic and morphologic characteristic of congenital obstruction of small intestine in newborn babiesMorphology of jejunum of experimental animals has identical structural changes with morphology of jejunum in newborn babies with congenital abnormalities of small intestine. Solving of the problems regarding malformations of small intestine in new born babies is actively needed to transfer to the aspect of preventive measures
Journal problems of biology and medicine -
 New generation stents coated with medicines, results of clinical triaThe advent of drug-eluting stents (DCTs) in the early 21st century has dramatically changed the strategy for revascularization in coronary artery disease. Target stenosis and large Dermatological coronary interventions with the use of DKS compared with conventional metal stents, due to a significant reduction in the frequency of re-interventions of cardiac complications of coronary heart disease (CHD) the strategy of revascularization quickly dominated in patients with. Despite the progress made using first generation DQS (Cypher, Taxus)the frequency of severe cardiac complications (mortality, myocardial infarction, re-injury) remained high for 5 years and approached 20% [1]. The main problems of the first generation DQS era were manifested in late and very late stent thrombosis, as well as late resolution of vascular perforation. First generation DQS These "shortcomings" forced manufacturers to create a new generation of DQS.Больше информации об этом исходном текстеЧтобы получить дополнительную информацию, введите исходный текст Отправить отзывБоковые панели
New generation stents coated with medicines, results of clinical triaThe advent of drug-eluting stents (DCTs) in the early 21st century has dramatically changed the strategy for revascularization in coronary artery disease. Target stenosis and large Dermatological coronary interventions with the use of DKS compared with conventional metal stents, due to a significant reduction in the frequency of re-interventions of cardiac complications of coronary heart disease (CHD) the strategy of revascularization quickly dominated in patients with. Despite the progress made using first generation DQS (Cypher, Taxus)the frequency of severe cardiac complications (mortality, myocardial infarction, re-injury) remained high for 5 years and approached 20% [1]. The main problems of the first generation DQS era were manifested in late and very late stent thrombosis, as well as late resolution of vascular perforation. First generation DQS These "shortcomings" forced manufacturers to create a new generation of DQS.Больше информации об этом исходном текстеЧтобы получить дополнительную информацию, введите исходный текст Отправить отзывБоковые панели
Journal problems of biology and medicine -
 Surgical correction of complications of ritual circumcision of prepuceat homeThe peculiarity of manycountries, is a ritual circumcision of prepuce, it is often carried out at home by people without medical training, without regard to the rules of asepsis and antisepsis, anatomy of the body, assessing the overall status and comorbidities. One of the serious complications that lead to disability is cut-ting off a part of glans penis along with part of foreskin, these patients will suffer from cicatrical stenosis of the external foramen of the urethra in the future for a long time. In urology department PSRSSPMCP is be-ing treated 35 children aged 1 to 8 years with a diagnosis of cicatricial narrowing of the external foramen of the urethra after the ritual circumcision at home. In the urology department implemented method of surgical treatment of cicatricial narrowing of the external foramen of the urethra, which was used in all 35 patients. The results of treatment were studied in all patients within 6 months. up to 1.5 years, with no observed re-lapse. The proposed method of surgical correction of cicatricial stenosis of the external foramen of the ure-thra is simple; the risk of recurrence is minimal.
Surgical correction of complications of ritual circumcision of prepuceat homeThe peculiarity of manycountries, is a ritual circumcision of prepuce, it is often carried out at home by people without medical training, without regard to the rules of asepsis and antisepsis, anatomy of the body, assessing the overall status and comorbidities. One of the serious complications that lead to disability is cut-ting off a part of glans penis along with part of foreskin, these patients will suffer from cicatrical stenosis of the external foramen of the urethra in the future for a long time. In urology department PSRSSPMCP is be-ing treated 35 children aged 1 to 8 years with a diagnosis of cicatricial narrowing of the external foramen of the urethra after the ritual circumcision at home. In the urology department implemented method of surgical treatment of cicatricial narrowing of the external foramen of the urethra, which was used in all 35 patients. The results of treatment were studied in all patients within 6 months. up to 1.5 years, with no observed re-lapse. The proposed method of surgical correction of cicatricial stenosis of the external foramen of the ure-thra is simple; the risk of recurrence is minimal.
Journal problems of biology and medicine -
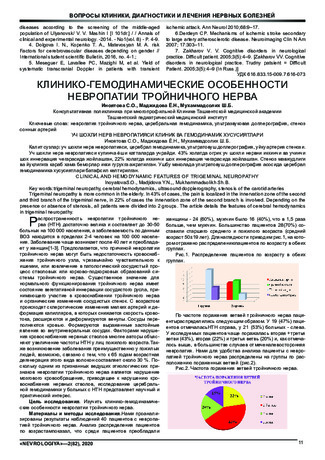
Trigeminal neuropathy is more common in the elderly. In 43% of cases, the pain is localized in the innervation zone of the second and third branch of the trigeminal nerve, in 22% of cases the innervation zone of the second branch is involved. Depending on the presence or absence of stenosis, all patients were divided into 2 groups. The article details the features of cerebral hemodynamics in trigeminal neuropathy.
-
 Comporative analysis of the results of surgical treatment of patients with bile duct syndrome after cholecystectomyAnalyzed treatment results 72 patients with the closest postoperative period after cholecystectomy. In the studied groups, the frequency and sources of postoperative bile leakage, as well as the nature and localization of injuries of the breast, at the onset of bile, 1 degree, drainage were studied or delimited accumulations of fluid in projection of the gallbladder bladder not more than 5 cm according to the ultrasound, as well as in a satisfactory condition of the patient, no symptoms irritation peritoneum and changes in blood analysis adhered to tactics active dynamic observed with mandatory ultrasonic control. At the expiration of bile by drainage 2 degrees performed ERCP. The main operation at complete intersection and excision of the extrahepatic bile ducts is HepEA; with well distant result in 95.3%. Restorative operation shown only with partial damage to the ductus.
Comporative analysis of the results of surgical treatment of patients with bile duct syndrome after cholecystectomyAnalyzed treatment results 72 patients with the closest postoperative period after cholecystectomy. In the studied groups, the frequency and sources of postoperative bile leakage, as well as the nature and localization of injuries of the breast, at the onset of bile, 1 degree, drainage were studied or delimited accumulations of fluid in projection of the gallbladder bladder not more than 5 cm according to the ultrasound, as well as in a satisfactory condition of the patient, no symptoms irritation peritoneum and changes in blood analysis adhered to tactics active dynamic observed with mandatory ultrasonic control. At the expiration of bile by drainage 2 degrees performed ERCP. The main operation at complete intersection and excision of the extrahepatic bile ducts is HepEA; with well distant result in 95.3%. Restorative operation shown only with partial damage to the ductus.
Doctor's Herald -
 Neurohistological methods found polyvalent receptors in the wall of various designs biliary systems. The concentration of receptor structures of the highest in the end of the common bile duct, including vials of fater papilla. In this area the receptors overlap each other and form the receptor field. The basic amount of receptor sites associated with spinal 7-8 thoracic segments of the spinal cord.
Neurohistological methods found polyvalent receptors in the wall of various designs biliary systems. The concentration of receptor structures of the highest in the end of the common bile duct, including vials of fater papilla. In this area the receptors overlap each other and form the receptor field. The basic amount of receptor sites associated with spinal 7-8 thoracic segments of the spinal cord. -
 Mirizzi syndrome (MS) is one of the least understood concepts in bile duct surgery. This is due to the rarity of this pathology. This disease occurs according to the literature, from 0.5 to 5% among all patients operated on for gallstone disease [6, 12, 13, 17]. In connection with the progress of biliary tract surgery, an increase in the incidence of cholelithiasis, interest in this problem has increased in recent years. However, there is still no consensus on the diagnosis and tactics of surgical treatment [1, 2, 7, 15]. MS is often diagnosed only during surgery, which increases the percentage of access conversion and the risk of trauma to the common bile duct [9, 18].
Mirizzi syndrome (MS) is one of the least understood concepts in bile duct surgery. This is due to the rarity of this pathology. This disease occurs according to the literature, from 0.5 to 5% among all patients operated on for gallstone disease [6, 12, 13, 17]. In connection with the progress of biliary tract surgery, an increase in the incidence of cholelithiasis, interest in this problem has increased in recent years. However, there is still no consensus on the diagnosis and tactics of surgical treatment [1, 2, 7, 15]. MS is often diagnosed only during surgery, which increases the percentage of access conversion and the risk of trauma to the common bile duct [9, 18]. -
 Нейрогистологическая картина приступа острой боли при заболеваниях желчевыделительной системы
Нейрогистологическая картина приступа острой боли при заболеваниях желчевыделительной системы
Prospects for the development of medicineНарушение двигательной функции желчных протоков, проявляющееся нарушением отведения желчи из печени или желчного пузыря в 12- перстную кишку ведет к развитию различных типов дискенезии желчевыводящих путей, которые могут осложниться желчнокаменной болезнью. Самым первым симптомом будет боль, так как области протока сосредоточено множество нервных окончаний.
-
 FUNDAMENTALS OF RADIATION DIAGNOSTICS OF THE HEART AND LARGE VESSELS IN CHILDREN (REVIEW)Radiation diagnostics of the heart and large vessels in children are part of the general clinical examination of the patient. Its purpose is to establish a diagnosis of the disease, as well as determine the nature of hemodynamic disorders. The examination plan (algorithm) of children should be drawn up in such a way as to avoid excessive exposure. X-ray endovascular interventions include many other manipulations: scabbard, scabbard closure of uninhabited arterial duct Batalov and defect in the septum of the heart, scabbard embolectomy, scabbard removal of foreign bodies from the heart. This technique is used in chemotherapy to dissolve blood clots in the lumen of the vasodilatation thrombolysis. New endovascular manipulations are, first of all, the introduction of a special filter transcatheter method in the hollow and femoral veins to prevent thromboembolism of the branches of the pulmonary artery in varicose veins of the limbs, such as thrombophlebitis. Secondly, the introduction of a "memory" vessel into the endoprosthesis vessel and the use of a flexible light probe for laser destruction of atheromatous plaques and clots.
FUNDAMENTALS OF RADIATION DIAGNOSTICS OF THE HEART AND LARGE VESSELS IN CHILDREN (REVIEW)Radiation diagnostics of the heart and large vessels in children are part of the general clinical examination of the patient. Its purpose is to establish a diagnosis of the disease, as well as determine the nature of hemodynamic disorders. The examination plan (algorithm) of children should be drawn up in such a way as to avoid excessive exposure. X-ray endovascular interventions include many other manipulations: scabbard, scabbard closure of uninhabited arterial duct Batalov and defect in the septum of the heart, scabbard embolectomy, scabbard removal of foreign bodies from the heart. This technique is used in chemotherapy to dissolve blood clots in the lumen of the vasodilatation thrombolysis. New endovascular manipulations are, first of all, the introduction of a special filter transcatheter method in the hollow and femoral veins to prevent thromboembolism of the branches of the pulmonary artery in varicose veins of the limbs, such as thrombophlebitis. Secondly, the introduction of a "memory" vessel into the endoprosthesis vessel and the use of a flexible light probe for laser destruction of atheromatous plaques and clots.
Journal of Cardiorespiratory Research -
 Histological structure of the intramural nervous apparatus of the general gall bladder and gall bladder in the rabbit, in normality and after gall bladder removal
Histological structure of the intramural nervous apparatus of the general gall bladder and gall bladder in the rabbit, in normality and after gall bladder removal
Journal of Biomedicine and PracticeThe histological structure of the extrahepatic bile ducts in rabbits in normal conditions and after removal of the gallbladder.
-
 Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Catalog of abstractsRelevance of the problem.Despite the great successes of angiosurgery, the problem of surgical treatment of abdominal aortic aneurysms does not lose its relevance. World health statistics records a steady increase in the incidence of abdominal aortic aneurysm (ABA). According to L.J. Melton et al. (1984) and L.K. Bickerstaff et al. (1984) in the USA the number of patients with abdominal aortic aneurysm has increased 7 times in 30 years since 1951. In England and Wales, according to F.G. Fowkers et al. (1989) for the same period revealed a 20-fold increase in abdominal aortic aneurysms in men and 11-fold in women. According to the results of multicentre screening studies ABA was detected in 8% of the examined (E.S. Vourvouri, 2001), and in the age group of 64-69 years ABA was detected in 5.7% of the examined, and in the age group of 75-81 years - in 8.9% (R.A.P. Skott et al., 2001). A similar trend is observed in other countries. Accordingly, mortality from ABA is also increasing - aneurysm rupture in a number of countries is one of the ten most frequent causes of death among elderly and senile people (F.A. Lederle et al., 1990)
Currently, planned aneurysm resection has become a recognised standard of radical treatment of ABA patients and the number of these operations is steadily increasing. For example, about 40,000 ABA resections are performed annually in the USA (J.J. Grange et al., 1997). In Sweden during the period from 1987-89 to 1993-95 the number of ABA operations increased 5 times and currently 10 operations per 100,000 population are performed (A.Hallin et al., 2001), although this is 1.5 - 2 times less than the required number. However, postoperative lethality is still quite high and makes 5-7% (A.V.Pokrovskiy et al., 1992; Y.V.Belov et al., 1992; V.V.Vakhidov et al., 1992; A.W. Bradbury et al. Bradbury et al., 1997; A.Hallin et al., 2001).
E.W. Steyeberg et al. (1995) summarised the data of literature on 17238 ABA resection operations and gave an average mortality of 6.8%.
Multicentre studies in five major hospitals in the Netherlands found that only 74% of patients underwent ABA resection without complications; 26% had some complications, 9% of which were severe and 4.1% of which were fatal (G.J. Akkersdijk et al., 1998). Similar results were obtained in the Canadian Cooperative Study (K.W. Johnston et al., 1990). It was established that the peculiarity of complications in the majority of patients was their systemic character (L.L. Lau et al, 2001) The course of the postoperative period is most often complicated by cardiac, respiratory, renal, cerebrovascular, as well as complications associated with thrombosis and bleeding (W.E. Lloyd et al., 1996; R.D. Sayers et al., 1997; J.D. Blankenstein et al., 1998; R. Ayari et al., 1998). Ayari et al., 2001)
The undisputed leadership, without doubt, belongs to cardiac complications, the incidence of which varies from 10% to 20%. Moreover, cardiac complications account for 50-70% of total mortality. Cerebrovascular complications, although not uncommon, account for no more than 1-1.5%, but their mortality reaches 40%. Complications associated with thromboses and haemorrhages in the perioperative period reach 2-5% (M.M.Reigel et al., 1987; K.W.Johnson et al., 1990; N.Franklin et al., 1993; A.A.Milne et al., 1994).
Certainly, a large number of complications after resection of abdominal aortic aneurysms is caused by the initial severity of patients' condition, however, many unresolved tactical and technical issues of patients' preparation for the operation, stage of performance in case of combined lesions of several vascular basins play a practically significant role. Adequate management of the operation itself and the immediate postoperative period is no less important, taking into account the possibility of such dreadful complications as thrombosis and embolism, cerebral and cardiac death. Until now there is no unified complex analysis of the results of treatment of uncomplicated abdominal aortic aneurysms and, accordingly, recommendations for the prevention of possible complications.
All this determined our aim and objectives of the study.
The aim of the study is to improve the results of surgical treatment of ABA by developing an effective system for determining the main risk factors of surgical treatment and optimal surgical tactics to prevent possible complications.
Scientific novelty.For the first time a complex analysis of indications and contraindications to surgical treatment of abdominal aortic aneurysms was carried out
The most significant concomitant pathology capable to lead to formidable complications and lethality during the intervention and in the nearest postoperative period was revealed. Adequate measures of their prevention and treatment were proposed.
The algorithm of surgical treatment tactics for patients with combined pathology of coronary arteries and aortic arch branch lesions was developed
The state of haemostasis system at all stages of reconstructive surgery on abdominal aorta, starting from skin incision to wound closure, was studied for the first time.
Conclusions:
1. The proposed original classification of ABA, based on mutual dependence on the etiology of the disease, localisation, concomitant diseases, clinic and its course, allows to determine the strategy of early diagnosis, to estimate the most significant risk factors, the stage of intervention in combined lesions of adjacent and distant vascular basins and, ultimately, to determine the ways to reduce complications and mortality in patients with ABA.
2. The most informative methods of ABA diagnostics are duplex scanning and computed tomography. Non-invasive diagnostics capabilities are enough to determine the aneurysm size, its relation to the renal arteries, as well as to find out the state of visceral branches and aortic bifurcation. Abdominal aortography is indicated in patients with concomitant arterial hypertension to identify the state of the renal arteries.
3. Significant risk factors in these patients are ischaemic heart disease (44.1%), arterial hypertension (49%), haemostasis disorders (almost 100%).
4. The leading concomitant disease in the development of postoperative complications is ischaemic heart disease. Its share in abdominal aortic aneurysms is 40%. Postoperative cardiac complications reach 14.9%. Diagnostics of ischaemic heart disease should be based on the stage-by-stage detection of coronary lesions and its functional-compensatory abilities.
5. The main complications of the postoperative period after ABA resections are acute heart failure (14,9%), cerebral circulatory disorders (1,5%), acute renal failure (3,33%).
6. When significant coronary vascular channel lesions are detected in patients with ABA, it is fundamental to solve the issue of intervention staging. At 3-4 functional classes of circulatory insufficiency, appearance of new zones of hypo- or akinesia, decrease of ejection fraction below 40%, the first stage should be myocardial revascularisation surgery
7. In patients with combined lesions of brachiocephalic vessels in patients with ABA it is reasonable to assess the cerebral blood flow. In the presence of 70% or more stenosis of VCA, presence of embologenic plaque, bilateral haemodynamically significant stenosis it is necessary to perform carotid artery intervention as the first stage.
8. One of the most difficult problems of reconstructive operations in ABA is the contiguous lesion of renal and visceral branches of the abdominal aorta. The principle is their one-stage reconstruction. The types of reconstruction of these branches should be variable depending on the volume and extent of the pathological process.
9. Patients with aneurysmal lesion of abdominal aorta initially always have significant disorders of haemostasis system. In 30% of patients with occlusive diseases of aorta and its branches in the preoperative period the activity of thrombocytic-vascular link of hemostasis is increased, antithrombotic ability of vascular wall endothelium is decreased and blood rheological properties are disturbed. Activation of fibrinolysis was noted in patients with aneurysmal lesion of abdominal aorta.
10. During the operation for abdominal aortic aneurysmal lesion, after starting the blood flow the level of plasminogen increases additionally by 30%, which is a risk factor for haemorrhagic complications in the perioperative period. On the 1-3 day after the operation there is a significant decrease of blood anticoagulant potential - antithrombin-Sh by 25-27%, protein C by 23-25%. This period is the most dangerous in terms of thrombohemorrhagic complications development.
11. When using standard heparin during the operation there is a consumption of antithrombin-Sh by 30-45% and increase of platelet aggregation by 10%, which is a threatening condition for the occurrence of thrombosis of deep veins of the lower extremities with subsequent TELA. When using fraxiparin during reconstructive vascular surgeries the consumption of antithrombin-Sh and increase in platelet aggregation do not occur, prothrombin time, activated partial thromboplastin time, thrombin time are lengthened insignificantly that testifies to expediency of its use for prevention of thrombohemorrhagic complications.
12. Application of the diagnostic methods proposed by us to detect the main risk factors during the operation and in the nearest postoperative period, use of the algorithm of stage and volume of intervention allowed to reduce significantly the number of threatening complications, thus the lethality decreased 4 times, and the number of non-fatal complications - 4 times non-fatal complications - 1.5 times. -
 Present study was to optimize the treatment of patients with subglottic laryngeal stenosis. Materials and methods: We have examined a total of 8 patients presenting with subglottic laryngeal stenosis. The etiological factors and underlying conditions of laryngeal stenosis were the prolonged intubation in 5 patients. Wegener granulomatosis in 3 patients. All the patients underwent balloon dilatation with the apphcation of the \ideo endoscopic technique. Results: The surgical treatment of all the patients made it possible to achieve the persistent expansion of the lumen of the subglottic part of the larynx, to shorten the periods of the in-patient treatment and rehabilitation of the patients. Restenosis of laryngeal lining stenting was observed in one patient presenting with Wegener’s granulomatosis which was associated with the relapse of the underlying disease.
Present study was to optimize the treatment of patients with subglottic laryngeal stenosis. Materials and methods: We have examined a total of 8 patients presenting with subglottic laryngeal stenosis. The etiological factors and underlying conditions of laryngeal stenosis were the prolonged intubation in 5 patients. Wegener granulomatosis in 3 patients. All the patients underwent balloon dilatation with the apphcation of the \ideo endoscopic technique. Results: The surgical treatment of all the patients made it possible to achieve the persistent expansion of the lumen of the subglottic part of the larynx, to shorten the periods of the in-patient treatment and rehabilitation of the patients. Restenosis of laryngeal lining stenting was observed in one patient presenting with Wegener’s granulomatosis which was associated with the relapse of the underlying disease. -
CLINICAL AND FUNCTIONAL STUDY OF PATIENTS WITH CHRONIC STENOSE OF THE LARYNXThe aim of the study was to increase the effectiveness of the treatment of patients with chronic scarring of the larynx through the use of new medical technologies and improve pre- and postoperative care. The study showed that the role of spirometry, endoscopy in the diagnosis of patients with narrowing of the larynx in the vocal cords and narrowing of the larynx in the vocal cords and trachea is important.
Medicine and innovations -
 New methods of laryngoplasty in patients with chronic paralytic stenosis of the larynxThe aim of the study was to evaluate the effectiveness of various types of surgical treatment of patients with bilateral paralytic stenosis of the larynx.The study involved 22 patients aged 2 to 60 years,suffering from paralytic stenosis of the larynx, who was treated in the period from 2015 to 2020. The results of treatment with the use of laser resection of the vocal fold, Closing the surgical wound with matching the edges of the mucous membrane and suturing provides fast healing by primary intention, which allows you to start early therapeutic and phonopedic rehabilitation.All this allows us to recommend laser submucosal chordaritenoidotomy for use in clinical practice.
New methods of laryngoplasty in patients with chronic paralytic stenosis of the larynxThe aim of the study was to evaluate the effectiveness of various types of surgical treatment of patients with bilateral paralytic stenosis of the larynx.The study involved 22 patients aged 2 to 60 years,suffering from paralytic stenosis of the larynx, who was treated in the period from 2015 to 2020. The results of treatment with the use of laser resection of the vocal fold, Closing the surgical wound with matching the edges of the mucous membrane and suturing provides fast healing by primary intention, which allows you to start early therapeutic and phonopedic rehabilitation.All this allows us to recommend laser submucosal chordaritenoidotomy for use in clinical practice.
Medicine and innovations