Library search
Search Results
-
 Firm deformations of the larynx and trachea: clinic-functional characteristic, optimization of treatment and early rehabilitation
Firm deformations of the larynx and trachea: clinic-functional characteristic, optimization of treatment and early rehabilitation
Catalog of abstractsSubject of the inquiry: 298 patients with finn deformations of the larynx and trachea
Aim of the inquiry: early rehabilitation of patients with firm deformations of the larynx and trachea path optimization and creating clinical and pathogenic methods of complex treatment.
Methods of the inquiry: clinical examination, special examination: LOR-examination, endoscopy of air ways, X-ray, CT, MRI of larynx, trachea and bronchus, bacterial examination of larynx and trachea wounds; morphological examination, biochemical methods of examination: lipid peroxidation, antioxidant enzymes, activity of hepatic monooxygenase system (MOS); biophysical methods of examination: исследование electric damage of erythrocytes’ membrane (EDEM), blood viscosity (BV) and blood shift velocity (BSV); cytological examination.
The results achieved and their novelty: In patients with firm deformations of the larynx and trachea, firstly basing on complex investigation clinical and structural-functional parameters revealed pathomorphological changes in neck tissues as chronic inflammation with productive component. Despite, revealed disrupt balance of process lipid peroxidation and antioxidant system, hydroxylic function of liver, decrease of electoral penetrability of erythrocytes’ membrane and aggravate of hemorheology. With this, level of expression of changes depends on clinic form and load disease, correlate with stage of wound healing and after restore of functions of the larynx and trachea gradually becoming normal. Presented classification of the firm deformations of the larynx and trachea, permitting complexly counting etiologic factor and morphological variant of the damage of laryngotracheal tract. In scheme of the pathogenic complex conservative therapy before and after reconstructive operations included medicine, influencing on Hemodynamic, with ability membranotrope action, systemic enzymotherapy, immunostimulators, and correction of the tissue metabolism by laser. Created private and modified methods of reconstructive laryngotracheoplasty in case of cicatricle stenosis of glottic and subglottic parts, bilateral paralyses of the larynx, cicatricle deformations of pharyngolarynx, combination deformations and defects of the larynx and trachea, permitting single stage restore laryngotracheal ways.
Practical value: The investigation of pathogenic mechanism of developing of the firm deformations of the larynx and trachea on data of changes of main functional and metabolic processes will permit not only activating and improving of pathogenic therapy, and forecasting variant of development and course of postoperative period after reconstructive operations.
Use of proposed methods of complex conservative and surgical treatment of the firm deformations of the larynx and trachea allowed to provide whole volume of restoring means in more short time and with less quantity of stage operations, preoperative preparing till 3 days, hospital stay till 14-20 days, surgical operations in 1.9 time.
Degree of embed and economical effectivity: The results of investigation intruded in treatment practice of the First and Second Tashkent Medical Institutes, LOR-clinics of Samarqand territorial children hospital, territorial hospital of Karshi. Materials of the investigation using in study process of LOR - cathedra First Tashkent Medical Institutes during lectures and practice tutorials with students, magistracies, and clinic ordinators. Determined main economic effect in use of proposed complex therapy in connection with reduce of term of treatment and hospital stay (on an average 10 days) and taking off or decreased disability on 67% patients.
Sphere of usage: otorhinolaryngology, surgery, reanimation -
 Present study was to optimize the treatment of patients with subglottic laryngeal stenosis. Materials and methods: We have examined a total of 8 patients presenting with subglottic laryngeal stenosis. The etiological factors and underlying conditions of laryngeal stenosis were the prolonged intubation in 5 patients. Wegener granulomatosis in 3 patients. All the patients underwent balloon dilatation with the apphcation of the \ideo endoscopic technique. Results: The surgical treatment of all the patients made it possible to achieve the persistent expansion of the lumen of the subglottic part of the larynx, to shorten the periods of the in-patient treatment and rehabilitation of the patients. Restenosis of laryngeal lining stenting was observed in one patient presenting with Wegener’s granulomatosis which was associated with the relapse of the underlying disease.
Present study was to optimize the treatment of patients with subglottic laryngeal stenosis. Materials and methods: We have examined a total of 8 patients presenting with subglottic laryngeal stenosis. The etiological factors and underlying conditions of laryngeal stenosis were the prolonged intubation in 5 patients. Wegener granulomatosis in 3 patients. All the patients underwent balloon dilatation with the apphcation of the \ideo endoscopic technique. Results: The surgical treatment of all the patients made it possible to achieve the persistent expansion of the lumen of the subglottic part of the larynx, to shorten the periods of the in-patient treatment and rehabilitation of the patients. Restenosis of laryngeal lining stenting was observed in one patient presenting with Wegener’s granulomatosis which was associated with the relapse of the underlying disease. -
 This article presents the issues of surgical reconstruction of the larynx in injuries of the thyroid membrane. We use two types of thyrohyoidopexy in case of injuries of the thwoid membrane. In the first version of surgery. we perform in the early period after an open or closed injur,' of the thyroid membrane. The second version of the surgery is used in case of old closed injuries of the thyroid membrane, that is. when the persistent effects of this injury are stated as a scarry stenosis of the larynx with a defect in the front wall. In order to well mobilize the larynx, it is enough to cut only the sternothyroid muscles, and others use for better fixation of the anastomosis. In case of persistent effects of the old injuries of thyroid membrane, the method of choice can be the ability of the implantation of fragment of the body of the hyoid bone and the epiglottis into the cleft thyroid cartilage.
This article presents the issues of surgical reconstruction of the larynx in injuries of the thyroid membrane. We use two types of thyrohyoidopexy in case of injuries of the thwoid membrane. In the first version of surgery. we perform in the early period after an open or closed injur,' of the thyroid membrane. The second version of the surgery is used in case of old closed injuries of the thyroid membrane, that is. when the persistent effects of this injury are stated as a scarry stenosis of the larynx with a defect in the front wall. In order to well mobilize the larynx, it is enough to cut only the sternothyroid muscles, and others use for better fixation of the anastomosis. In case of persistent effects of the old injuries of thyroid membrane, the method of choice can be the ability of the implantation of fragment of the body of the hyoid bone and the epiglottis into the cleft thyroid cartilage. -
 Доброкачественные опухоли гортани (ДОГ) составляют 1-2% от общего количества заболеваний гортани (1). Хондрома - опухоль из оформленной соединительной ткани, растущая из хондробластов и представляющая собой искаженный хрящ с беспорядочной структурой. В 1822 г. Об обнаружении хрящевой опухали в гортани сообщил Нсунсигср (цит. По А. И. Пачсс (3)). Хондромы гортани (ХГ) состоят из зрелой хрящевой ткани, как правило, гиалиновой. Хрящевые капсулы распределяются неравномерно, они крупнее обычных, включают кос - где сразу 2- 3 клетки.
Доброкачественные опухоли гортани (ДОГ) составляют 1-2% от общего количества заболеваний гортани (1). Хондрома - опухоль из оформленной соединительной ткани, растущая из хондробластов и представляющая собой искаженный хрящ с беспорядочной структурой. В 1822 г. Об обнаружении хрящевой опухали в гортани сообщил Нсунсигср (цит. По А. И. Пачсс (3)). Хондромы гортани (ХГ) состоят из зрелой хрящевой ткани, как правило, гиалиновой. Хрящевые капсулы распределяются неравномерно, они крупнее обычных, включают кос - где сразу 2- 3 клетки. -
CLINICAL AND FUNCTIONAL STUDY OF PATIENTS WITH CHRONIC STENOSE OF THE LARYNXThe aim of the study was to increase the effectiveness of the treatment of patients with chronic scarring of the larynx through the use of new medical technologies and improve pre- and postoperative care. The study showed that the role of spirometry, endoscopy in the diagnosis of patients with narrowing of the larynx in the vocal cords and narrowing of the larynx in the vocal cords and trachea is important.
Medicine and innovations -
 New methods of laryngoplasty in patients with chronic paralytic stenosis of the larynxThe aim of the study was to evaluate the effectiveness of various types of surgical treatment of patients with bilateral paralytic stenosis of the larynx.The study involved 22 patients aged 2 to 60 years,suffering from paralytic stenosis of the larynx, who was treated in the period from 2015 to 2020. The results of treatment with the use of laser resection of the vocal fold, Closing the surgical wound with matching the edges of the mucous membrane and suturing provides fast healing by primary intention, which allows you to start early therapeutic and phonopedic rehabilitation.All this allows us to recommend laser submucosal chordaritenoidotomy for use in clinical practice.
New methods of laryngoplasty in patients with chronic paralytic stenosis of the larynxThe aim of the study was to evaluate the effectiveness of various types of surgical treatment of patients with bilateral paralytic stenosis of the larynx.The study involved 22 patients aged 2 to 60 years,suffering from paralytic stenosis of the larynx, who was treated in the period from 2015 to 2020. The results of treatment with the use of laser resection of the vocal fold, Closing the surgical wound with matching the edges of the mucous membrane and suturing provides fast healing by primary intention, which allows you to start early therapeutic and phonopedic rehabilitation.All this allows us to recommend laser submucosal chordaritenoidotomy for use in clinical practice.
Medicine and innovations -
 Evaluation of the methods of the bed of adenoma processing with the purpose of hemostasis in prostate adenomectomyIt has been shown the complexity and difficulty of hemostasis as an important stage of prostate adenomectomy in benign prostate hyperplasia. Based on the hemostasis results study in prostate adenomectomy at 490 patients with variety of ways (tamponagc of the bed of adenoma - 398 patients, removable sutures imposition - 58, suturing of the bed - 22, using lagochilus water infusion -12 patients) shows that processing of the bed of adenoma with lagochilus and hydrostatic irrigation of the bladder has a number of advantages of this local hemostatic. In addition, optimal conditions for natural reduction and formation of the bladder neck (the bed of adenoma) after adenomectomy arc being created in compare with strains after tamponage, bringing down or suturing.
Evaluation of the methods of the bed of adenoma processing with the purpose of hemostasis in prostate adenomectomyIt has been shown the complexity and difficulty of hemostasis as an important stage of prostate adenomectomy in benign prostate hyperplasia. Based on the hemostasis results study in prostate adenomectomy at 490 patients with variety of ways (tamponagc of the bed of adenoma - 398 patients, removable sutures imposition - 58, suturing of the bed - 22, using lagochilus water infusion -12 patients) shows that processing of the bed of adenoma with lagochilus and hydrostatic irrigation of the bladder has a number of advantages of this local hemostatic. In addition, optimal conditions for natural reduction and formation of the bladder neck (the bed of adenoma) after adenomectomy arc being created in compare with strains after tamponage, bringing down or suturing.
Doctor's Herald -
 Study of the immune system of children with laryngeal papillomatosis on the background of antiviral therapyA comparative analysis of the immunological parameters in the dynamics (before and after) of standard therapy and after standard + immunotropic therapy was performed in 252 children with papillomatosis of the larynx at the age of 3 to 9 years who were on the examination and treatment in the surgical department of oto-rhinolaryngology TMA. in the state of immune response in laryngeal papillomatosis, unidirectional changes, most pronounced in children with continuously recurrent form of laryngeal papillomatosis, were revealed. In the dynamics of therapy, there was an improvement in the cellular and humoral immunity, improvement in the clinical state of children, and a decrease in the frequency of relapses.
Study of the immune system of children with laryngeal papillomatosis on the background of antiviral therapyA comparative analysis of the immunological parameters in the dynamics (before and after) of standard therapy and after standard + immunotropic therapy was performed in 252 children with papillomatosis of the larynx at the age of 3 to 9 years who were on the examination and treatment in the surgical department of oto-rhinolaryngology TMA. in the state of immune response in laryngeal papillomatosis, unidirectional changes, most pronounced in children with continuously recurrent form of laryngeal papillomatosis, were revealed. In the dynamics of therapy, there was an improvement in the cellular and humoral immunity, improvement in the clinical state of children, and a decrease in the frequency of relapses.
Journal problems of biology and medicine -
 State of local mucosal immunity laryngeal children in normal and stenosing laryngotracheitis recurrentThe article presents the results of a study of the local features of mucosal immunity in the throat of healthy children from 2 months to 4 years. Noted that in healthy children coping mechanisms responding mucosal immune system is characterized by equi larynx involving cellular and humoral factors. In patients with acute, especially recurrent laryngotracheitis, laryngeal mucosal response characterized by activation of humoral factors (antibodies and WPA) absence of significant changes in the cellular immunity. There is a growing destructive processes affecting both epithelial and immune cells, neutrophils. Multiple relapses of acute laryngotracheitis in children determines a greater degree of immune response.
State of local mucosal immunity laryngeal children in normal and stenosing laryngotracheitis recurrentThe article presents the results of a study of the local features of mucosal immunity in the throat of healthy children from 2 months to 4 years. Noted that in healthy children coping mechanisms responding mucosal immune system is characterized by equi larynx involving cellular and humoral factors. In patients with acute, especially recurrent laryngotracheitis, laryngeal mucosal response characterized by activation of humoral factors (antibodies and WPA) absence of significant changes in the cellular immunity. There is a growing destructive processes affecting both epithelial and immune cells, neutrophils. Multiple relapses of acute laryngotracheitis in children determines a greater degree of immune response.
Journal problems of biology and medicine -
 On the base of studying and analyzing of modern literature and materials of forensic medicine expertise, connected with damage larynx complex, authors emphasized significant and unlearned aspects of these injured organs for task of forensic medicine expertise. It is marked, that practical forensic medicine expertise tasks re-quired further purposeful study of variety damage complex larynx, their systematization, and also elaborations of recommendation on determining degrees of severity, further damage, evaluations of trauma mechanism and thanatogenese of different types of enforced death in the complex of these damages
On the base of studying and analyzing of modern literature and materials of forensic medicine expertise, connected with damage larynx complex, authors emphasized significant and unlearned aspects of these injured organs for task of forensic medicine expertise. It is marked, that practical forensic medicine expertise tasks re-quired further purposeful study of variety damage complex larynx, their systematization, and also elaborations of recommendation on determining degrees of severity, further damage, evaluations of trauma mechanism and thanatogenese of different types of enforced death in the complex of these damages -
 FEATURES IN ASSESSING THE QUALITY OF VOICE IN CHILDREN WITH DYSPHONIAObjective: make a comparative analysis of the voice of the index (VHI) and endoscopic studies in the pathology of the voice of children. Material and Methods: The study involved 87 children, from 6 months to 14 years. The clinical study included fibrorinolaryngoscopy with video fixation (C-MAC, K.Storz, Ø-2,7 mm) and a survey of parents (or guardians) of children at the Uzbek version of the voice handicap index (pVHI), with sub-sections (functional - F, the physical - P and emotional - E). Results: endoscopic diagnosed laryngitis 20,6% (n = 18), functional 16,1% (n = 14) and mutational 9,2% (n = 8), dysphonia, benign larynx (respiratory papillamatosis) - 18.4 % (n = 16), the vocal cords paresis - 5.7% (n = 5), the vocal folds nodules 26.4% (n = 23), throat structure anomalies (acquired) 3,4% (n = 3). The survey revealed pVHI average points total pVHI and its sub-group of patients were as follows: F - 13,94, P - 15.48, E - 12.15 and T - 41.58, which is significantly higher than the group of healthy children and children with functional disorders of voice. Conclusions: Fibrolaryngoscopy with the smallest diameter of the lumen of the laryngoscope with video fixation allowed to quickly ascertain the diagnosis of organic disease of the larynx in children. In addition, the survey pVHI allowed to differentiate the severity of the vocal apparatus, to conduct timely special endoscopic diagnosis of vocal cord diseases.
FEATURES IN ASSESSING THE QUALITY OF VOICE IN CHILDREN WITH DYSPHONIAObjective: make a comparative analysis of the voice of the index (VHI) and endoscopic studies in the pathology of the voice of children. Material and Methods: The study involved 87 children, from 6 months to 14 years. The clinical study included fibrorinolaryngoscopy with video fixation (C-MAC, K.Storz, Ø-2,7 mm) and a survey of parents (or guardians) of children at the Uzbek version of the voice handicap index (pVHI), with sub-sections (functional - F, the physical - P and emotional - E). Results: endoscopic diagnosed laryngitis 20,6% (n = 18), functional 16,1% (n = 14) and mutational 9,2% (n = 8), dysphonia, benign larynx (respiratory papillamatosis) - 18.4 % (n = 16), the vocal cords paresis - 5.7% (n = 5), the vocal folds nodules 26.4% (n = 23), throat structure anomalies (acquired) 3,4% (n = 3). The survey revealed pVHI average points total pVHI and its sub-group of patients were as follows: F - 13,94, P - 15.48, E - 12.15 and T - 41.58, which is significantly higher than the group of healthy children and children with functional disorders of voice. Conclusions: Fibrolaryngoscopy with the smallest diameter of the lumen of the laryngoscope with video fixation allowed to quickly ascertain the diagnosis of organic disease of the larynx in children. In addition, the survey pVHI allowed to differentiate the severity of the vocal apparatus, to conduct timely special endoscopic diagnosis of vocal cord diseases.
Journal of oral medicine and craniofacial research -
 Результаты функционально сохранных операций при раке гортани распространенностью Т3
Результаты функционально сохранных операций при раке гортани распространенностью Т3
Actual problems of dentistry and maxillofacial surgery 4По современным рекомендациям разных международных онкологических обществ тактика лечения, т.е. выбор метода лечения на первом этапе рака гортани (РГ) существенно изменилась.
-
 Features of diagnosis and treatment of functional dysphonia in children
Features of diagnosis and treatment of functional dysphonia in children
Scientific works of gifted youth and medicine of the XXI centuryЗаболевания гортани, приводящие к нарушению голосовой функции, у детей, занимают по частоте второе место (20,3%) в структуре хронической патологии ЛОР - органов. Актуальность данной проблемы объясняется распространенностью, возрастанием частоты и переходом функциональных дисфоний в органическую дисфонию. При дальнейшем развитии ребенка, стойкое расстройство голосовой функции может приводить к ухудшению качества жизни, ограничению межличностных отношений, затруднению процесса социальной адаптации, что негативно отражается на общем развитии, нервно психическом состоянии и формировании личности ребенка. Тревожные, депрессивные расстройства могут способствовать развитию функциональной дисфоний. Значительную роль в возникновении функциональных дисфоний играют гормональные расстройства - чаще заболевания щитовидной железы. Другие причины - неврологические заболевания, такие, как болезнь Паркинсона и миастения, черепно-мозговая травма, нарушение мозгового кровообращения и др. Функциональные изменения обратимы, но в ряде случаев могут приводить к органическим изменениям гортани. Большинство исследователей связывают их с перенапряжением голоса.
-
 Ўткир бош мия қон томир патологиялари ривожланишида коллатерал қон билан таъминланишининг ўзига хослигининг аҳамияти
Ўткир бош мия қон томир патологиялари ривожланишида коллатерал қон билан таъминланишининг ўзига хослигининг аҳамияти
NeurologyБош мия қон-томир касалликлари тиббиётда ва иж тимоий ҳаётда долзарб муаммолардан бири бўлиб келмоқда. Ер юзида ЖССТ берган маълумотга кўра ҳар йили 15 млн.дан ортиқ аҳоли инсульт ташхиси билан рўйҳатга олинади, шуларнинг ярмидан кўпида 1 йил давомида ўлим ҳодисаси кузатилади. Тирик қолганларнинг 80%дан ортиғида ногиронлик келиб чиқади (27,26,19). Дастлабки 1-йилда инсульт ўтказганларнинг 5-25% ида қайта инсульт кузатилади, кейинги 5 йилда эса 20-40% беморларда кузатилади ( 21,8.). Такрорий инсульт натижасида эса 95-100% беморлар ногирон бўлиб қолишади ва уларнинг 65-80% и бегоналар ёрдамига мухтож бўладилар. 70% касалларда эса психик бузилишлар кузатилади (28). РАМН(РТФА) берган маълумотларга кўра ишемик инсульт(ИИ) билан касалланган беморларнинг 84,5% и 55 ёшдан юқори бўлган беморлар, эркаклар орасида бу кўрсаткич 40-55 ёшда 30% ни, аёллар орасида эса 40-60 ёшда 46,2% ни ташкил этади (6). Охирги йилларда инсультнинг бундай ёшариши бу муаммони нг долзарблигини янада оширмоқда.
-
 Epidemiologic and morphologic characteristic of congenital obstruction of small intestine in newborn babiesMorphology of jejunum of experimental animals has identical structural changes with morphology of jejunum in newborn babies with congenital abnormalities of small intestine. Solving of the problems regarding malformations of small intestine in new born babies is actively needed to transfer to the aspect of preventive measures
Epidemiologic and morphologic characteristic of congenital obstruction of small intestine in newborn babiesMorphology of jejunum of experimental animals has identical structural changes with morphology of jejunum in newborn babies with congenital abnormalities of small intestine. Solving of the problems regarding malformations of small intestine in new born babies is actively needed to transfer to the aspect of preventive measures
Journal problems of biology and medicine -
 New generation stents coated with medicines, results of clinical triaThe advent of drug-eluting stents (DCTs) in the early 21st century has dramatically changed the strategy for revascularization in coronary artery disease. Target stenosis and large Dermatological coronary interventions with the use of DKS compared with conventional metal stents, due to a significant reduction in the frequency of re-interventions of cardiac complications of coronary heart disease (CHD) the strategy of revascularization quickly dominated in patients with. Despite the progress made using first generation DQS (Cypher, Taxus)the frequency of severe cardiac complications (mortality, myocardial infarction, re-injury) remained high for 5 years and approached 20% [1]. The main problems of the first generation DQS era were manifested in late and very late stent thrombosis, as well as late resolution of vascular perforation. First generation DQS These "shortcomings" forced manufacturers to create a new generation of DQS.Больше информации об этом исходном текстеЧтобы получить дополнительную информацию, введите исходный текст Отправить отзывБоковые панели
New generation stents coated with medicines, results of clinical triaThe advent of drug-eluting stents (DCTs) in the early 21st century has dramatically changed the strategy for revascularization in coronary artery disease. Target stenosis and large Dermatological coronary interventions with the use of DKS compared with conventional metal stents, due to a significant reduction in the frequency of re-interventions of cardiac complications of coronary heart disease (CHD) the strategy of revascularization quickly dominated in patients with. Despite the progress made using first generation DQS (Cypher, Taxus)the frequency of severe cardiac complications (mortality, myocardial infarction, re-injury) remained high for 5 years and approached 20% [1]. The main problems of the first generation DQS era were manifested in late and very late stent thrombosis, as well as late resolution of vascular perforation. First generation DQS These "shortcomings" forced manufacturers to create a new generation of DQS.Больше информации об этом исходном текстеЧтобы получить дополнительную информацию, введите исходный текст Отправить отзывБоковые панели
Journal problems of biology and medicine -
 Surgical correction of complications of ritual circumcision of prepuceat homeThe peculiarity of manycountries, is a ritual circumcision of prepuce, it is often carried out at home by people without medical training, without regard to the rules of asepsis and antisepsis, anatomy of the body, assessing the overall status and comorbidities. One of the serious complications that lead to disability is cut-ting off a part of glans penis along with part of foreskin, these patients will suffer from cicatrical stenosis of the external foramen of the urethra in the future for a long time. In urology department PSRSSPMCP is be-ing treated 35 children aged 1 to 8 years with a diagnosis of cicatricial narrowing of the external foramen of the urethra after the ritual circumcision at home. In the urology department implemented method of surgical treatment of cicatricial narrowing of the external foramen of the urethra, which was used in all 35 patients. The results of treatment were studied in all patients within 6 months. up to 1.5 years, with no observed re-lapse. The proposed method of surgical correction of cicatricial stenosis of the external foramen of the ure-thra is simple; the risk of recurrence is minimal.
Surgical correction of complications of ritual circumcision of prepuceat homeThe peculiarity of manycountries, is a ritual circumcision of prepuce, it is often carried out at home by people without medical training, without regard to the rules of asepsis and antisepsis, anatomy of the body, assessing the overall status and comorbidities. One of the serious complications that lead to disability is cut-ting off a part of glans penis along with part of foreskin, these patients will suffer from cicatrical stenosis of the external foramen of the urethra in the future for a long time. In urology department PSRSSPMCP is be-ing treated 35 children aged 1 to 8 years with a diagnosis of cicatricial narrowing of the external foramen of the urethra after the ritual circumcision at home. In the urology department implemented method of surgical treatment of cicatricial narrowing of the external foramen of the urethra, which was used in all 35 patients. The results of treatment were studied in all patients within 6 months. up to 1.5 years, with no observed re-lapse. The proposed method of surgical correction of cicatricial stenosis of the external foramen of the ure-thra is simple; the risk of recurrence is minimal.
Journal problems of biology and medicine -
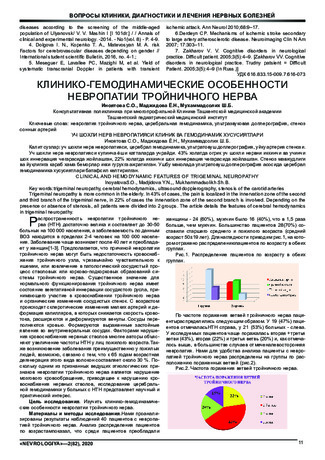
Trigeminal neuropathy is more common in the elderly. In 43% of cases, the pain is localized in the innervation zone of the second and third branch of the trigeminal nerve, in 22% of cases the innervation zone of the second branch is involved. Depending on the presence or absence of stenosis, all patients were divided into 2 groups. The article details the features of cerebral hemodynamics in trigeminal neuropathy.
-
The human thyroid gland is an unpaired organ consisting of two lobes connected by an isthmus. Normally, the thyroid gland is located on the anterior surface of the neck, fixed to the anterior and lateral surfaces of the trachea and larynx with connective tissue. The cells of the thyroid gland have a dual origin.
-
 In the department of head and neck tumors of the Tashkent regional oncological dispensary complex treatment of locally spread laryngopharyngeal cancer is performed witli the use of the combined operation «Laryngopharyngoesophagectomy witli one-stage pharyngoesophagoplasty with the help of the gastric stem». Despite the traumatism and high risk of postoperative complications, laryngopharyngoezofagectomy with a one-stage gastric stem plasty and pharyngogastroanastomosis is an alternative treatment of locally spread forms of cancer of the laryngopharynx and cervical esophagus resistant to chemoradiotherapy.
In the department of head and neck tumors of the Tashkent regional oncological dispensary complex treatment of locally spread laryngopharyngeal cancer is performed witli the use of the combined operation «Laryngopharyngoesophagectomy witli one-stage pharyngoesophagoplasty with the help of the gastric stem». Despite the traumatism and high risk of postoperative complications, laryngopharyngoezofagectomy with a one-stage gastric stem plasty and pharyngogastroanastomosis is an alternative treatment of locally spread forms of cancer of the laryngopharynx and cervical esophagus resistant to chemoradiotherapy. -
 MODERN METHODS OF TREATMENT OF CATARRHAL GINGIVITIS IN CHILDREN WITH DISABILITIESFrom periodontal pathologies to children with disabilities, the most common are inflammatory periodontal diseases - chronic catarrhal gingivitis. Chronic catarrhal gingivitis is a specific inflammatory process that is formed due to the concomitant effects of various EXO- and endogenous factors on the periodontal. The results of many researchers indicate that chronic infection in the soft tissues of the periodontal cavity and the health of the entire body is one of the extremely adverse consequences of inflammatory processes and increased risk factors leading to the transition of parallel catarrhal gingivitis into severe and intractable - ocular periodontitis.
MODERN METHODS OF TREATMENT OF CATARRHAL GINGIVITIS IN CHILDREN WITH DISABILITIESFrom periodontal pathologies to children with disabilities, the most common are inflammatory periodontal diseases - chronic catarrhal gingivitis. Chronic catarrhal gingivitis is a specific inflammatory process that is formed due to the concomitant effects of various EXO- and endogenous factors on the periodontal. The results of many researchers indicate that chronic infection in the soft tissues of the periodontal cavity and the health of the entire body is one of the extremely adverse consequences of inflammatory processes and increased risk factors leading to the transition of parallel catarrhal gingivitis into severe and intractable - ocular periodontitis.
Medicine and innovations -
 DIAGNOSIS OF CATARRHAL GINGIVITIS IN CHILDREN WITH DISABILITIESToday, one of the important tasks of providing dental care to disabled children with disabilities is limited on a global scale. From periodontal pathologies to children with disabilities, the most common are inflammatory periodontal diseases - chronic catarrhal gingivitis. Chronic catarrhal gingivitis is a specific inflammatory process that is formed due to the concomitant effects of various EXO- and endogenous factors on the periodontal. The results of many researchers indicate that chronic infection in the soft tissues of the periodontal cavity and the health of the entire body is one of the extremely adverse consequences of inflammatory processes and increased risk factors leading to the transition of parallel catarrhal gingivitis into severe and intractable - ocular periodontitis.
DIAGNOSIS OF CATARRHAL GINGIVITIS IN CHILDREN WITH DISABILITIESToday, one of the important tasks of providing dental care to disabled children with disabilities is limited on a global scale. From periodontal pathologies to children with disabilities, the most common are inflammatory periodontal diseases - chronic catarrhal gingivitis. Chronic catarrhal gingivitis is a specific inflammatory process that is formed due to the concomitant effects of various EXO- and endogenous factors on the periodontal. The results of many researchers indicate that chronic infection in the soft tissues of the periodontal cavity and the health of the entire body is one of the extremely adverse consequences of inflammatory processes and increased risk factors leading to the transition of parallel catarrhal gingivitis into severe and intractable - ocular periodontitis.
Journal of oral medicine and craniofacial research -
 Chronic hypertrophic rhinitis lead to the breakdown of the normal functioning of the body because of a violation of respiratory function, leading to circulator}' and tissue hypoxia, biochemical disturbances, including lipid metabolism and activity of the antioxidant system, which is accompanied by the development of the inflammatory reaction of the nasal mucosa; breach of natural immunity, as well as organic lesions of the paranasal sinuses, pharynx, larynx, lower respiratory tract. The examination and treatment of patients with chronic hypertrophic rhinitis who after surgical treatment along with conventional treatment included medication elfunat (ethylmethylhydroxypyridine succinate). Use of the drug has contributed elftinat: reduction of postoperative inflammatory reaction region and improve the activity of reparative tissue of the nose, the normalization of blood lipid peroxidation system and morpho-functional restoration layer of nasal mucosa.
Chronic hypertrophic rhinitis lead to the breakdown of the normal functioning of the body because of a violation of respiratory function, leading to circulator}' and tissue hypoxia, biochemical disturbances, including lipid metabolism and activity of the antioxidant system, which is accompanied by the development of the inflammatory reaction of the nasal mucosa; breach of natural immunity, as well as organic lesions of the paranasal sinuses, pharynx, larynx, lower respiratory tract. The examination and treatment of patients with chronic hypertrophic rhinitis who after surgical treatment along with conventional treatment included medication elfunat (ethylmethylhydroxypyridine succinate). Use of the drug has contributed elftinat: reduction of postoperative inflammatory reaction region and improve the activity of reparative tissue of the nose, the normalization of blood lipid peroxidation system and morpho-functional restoration layer of nasal mucosa. -
 Early diagnosis and treatment of children with hypertension-hydrocephalus against the background of long-term childbirthAccording to the literature, all injuries of the perinatal period are conditionally divided into hypoxic-ischemic (in which the lack of oxygen in the body is mainly brain structures), traumatic and mixed origin. As a result, the most common syndrome of encephalopathy is hypertension-hydrocephalus syndrome, which is manifested by an increase in spinal fluid and disruption of the liquor ducts. Hypertensive-hydrocephalus syndrome is manifested by disruption and swelling of the larynx, in some cases, the separation of the skull sutures, stiffness of the neck muscles.
Early diagnosis and treatment of children with hypertension-hydrocephalus against the background of long-term childbirthAccording to the literature, all injuries of the perinatal period are conditionally divided into hypoxic-ischemic (in which the lack of oxygen in the body is mainly brain structures), traumatic and mixed origin. As a result, the most common syndrome of encephalopathy is hypertension-hydrocephalus syndrome, which is manifested by an increase in spinal fluid and disruption of the liquor ducts. Hypertensive-hydrocephalus syndrome is manifested by disruption and swelling of the larynx, in some cases, the separation of the skull sutures, stiffness of the neck muscles.
Journal of hepato-gastroenterological research -
 Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Risk factors and their influence on the immediate results of surgical treatment of uncomplicated abdominal aortic aneurysms
Catalog of abstractsRelevance of the problem.Despite the great successes of angiosurgery, the problem of surgical treatment of abdominal aortic aneurysms does not lose its relevance. World health statistics records a steady increase in the incidence of abdominal aortic aneurysm (ABA). According to L.J. Melton et al. (1984) and L.K. Bickerstaff et al. (1984) in the USA the number of patients with abdominal aortic aneurysm has increased 7 times in 30 years since 1951. In England and Wales, according to F.G. Fowkers et al. (1989) for the same period revealed a 20-fold increase in abdominal aortic aneurysms in men and 11-fold in women. According to the results of multicentre screening studies ABA was detected in 8% of the examined (E.S. Vourvouri, 2001), and in the age group of 64-69 years ABA was detected in 5.7% of the examined, and in the age group of 75-81 years - in 8.9% (R.A.P. Skott et al., 2001). A similar trend is observed in other countries. Accordingly, mortality from ABA is also increasing - aneurysm rupture in a number of countries is one of the ten most frequent causes of death among elderly and senile people (F.A. Lederle et al., 1990)
Currently, planned aneurysm resection has become a recognised standard of radical treatment of ABA patients and the number of these operations is steadily increasing. For example, about 40,000 ABA resections are performed annually in the USA (J.J. Grange et al., 1997). In Sweden during the period from 1987-89 to 1993-95 the number of ABA operations increased 5 times and currently 10 operations per 100,000 population are performed (A.Hallin et al., 2001), although this is 1.5 - 2 times less than the required number. However, postoperative lethality is still quite high and makes 5-7% (A.V.Pokrovskiy et al., 1992; Y.V.Belov et al., 1992; V.V.Vakhidov et al., 1992; A.W. Bradbury et al. Bradbury et al., 1997; A.Hallin et al., 2001).
E.W. Steyeberg et al. (1995) summarised the data of literature on 17238 ABA resection operations and gave an average mortality of 6.8%.
Multicentre studies in five major hospitals in the Netherlands found that only 74% of patients underwent ABA resection without complications; 26% had some complications, 9% of which were severe and 4.1% of which were fatal (G.J. Akkersdijk et al., 1998). Similar results were obtained in the Canadian Cooperative Study (K.W. Johnston et al., 1990). It was established that the peculiarity of complications in the majority of patients was their systemic character (L.L. Lau et al, 2001) The course of the postoperative period is most often complicated by cardiac, respiratory, renal, cerebrovascular, as well as complications associated with thrombosis and bleeding (W.E. Lloyd et al., 1996; R.D. Sayers et al., 1997; J.D. Blankenstein et al., 1998; R. Ayari et al., 1998). Ayari et al., 2001)
The undisputed leadership, without doubt, belongs to cardiac complications, the incidence of which varies from 10% to 20%. Moreover, cardiac complications account for 50-70% of total mortality. Cerebrovascular complications, although not uncommon, account for no more than 1-1.5%, but their mortality reaches 40%. Complications associated with thromboses and haemorrhages in the perioperative period reach 2-5% (M.M.Reigel et al., 1987; K.W.Johnson et al., 1990; N.Franklin et al., 1993; A.A.Milne et al., 1994).
Certainly, a large number of complications after resection of abdominal aortic aneurysms is caused by the initial severity of patients' condition, however, many unresolved tactical and technical issues of patients' preparation for the operation, stage of performance in case of combined lesions of several vascular basins play a practically significant role. Adequate management of the operation itself and the immediate postoperative period is no less important, taking into account the possibility of such dreadful complications as thrombosis and embolism, cerebral and cardiac death. Until now there is no unified complex analysis of the results of treatment of uncomplicated abdominal aortic aneurysms and, accordingly, recommendations for the prevention of possible complications.
All this determined our aim and objectives of the study.
The aim of the study is to improve the results of surgical treatment of ABA by developing an effective system for determining the main risk factors of surgical treatment and optimal surgical tactics to prevent possible complications.
Scientific novelty.For the first time a complex analysis of indications and contraindications to surgical treatment of abdominal aortic aneurysms was carried out
The most significant concomitant pathology capable to lead to formidable complications and lethality during the intervention and in the nearest postoperative period was revealed. Adequate measures of their prevention and treatment were proposed.
The algorithm of surgical treatment tactics for patients with combined pathology of coronary arteries and aortic arch branch lesions was developed
The state of haemostasis system at all stages of reconstructive surgery on abdominal aorta, starting from skin incision to wound closure, was studied for the first time.
Conclusions:
1. The proposed original classification of ABA, based on mutual dependence on the etiology of the disease, localisation, concomitant diseases, clinic and its course, allows to determine the strategy of early diagnosis, to estimate the most significant risk factors, the stage of intervention in combined lesions of adjacent and distant vascular basins and, ultimately, to determine the ways to reduce complications and mortality in patients with ABA.
2. The most informative methods of ABA diagnostics are duplex scanning and computed tomography. Non-invasive diagnostics capabilities are enough to determine the aneurysm size, its relation to the renal arteries, as well as to find out the state of visceral branches and aortic bifurcation. Abdominal aortography is indicated in patients with concomitant arterial hypertension to identify the state of the renal arteries.
3. Significant risk factors in these patients are ischaemic heart disease (44.1%), arterial hypertension (49%), haemostasis disorders (almost 100%).
4. The leading concomitant disease in the development of postoperative complications is ischaemic heart disease. Its share in abdominal aortic aneurysms is 40%. Postoperative cardiac complications reach 14.9%. Diagnostics of ischaemic heart disease should be based on the stage-by-stage detection of coronary lesions and its functional-compensatory abilities.
5. The main complications of the postoperative period after ABA resections are acute heart failure (14,9%), cerebral circulatory disorders (1,5%), acute renal failure (3,33%).
6. When significant coronary vascular channel lesions are detected in patients with ABA, it is fundamental to solve the issue of intervention staging. At 3-4 functional classes of circulatory insufficiency, appearance of new zones of hypo- or akinesia, decrease of ejection fraction below 40%, the first stage should be myocardial revascularisation surgery
7. In patients with combined lesions of brachiocephalic vessels in patients with ABA it is reasonable to assess the cerebral blood flow. In the presence of 70% or more stenosis of VCA, presence of embologenic plaque, bilateral haemodynamically significant stenosis it is necessary to perform carotid artery intervention as the first stage.
8. One of the most difficult problems of reconstructive operations in ABA is the contiguous lesion of renal and visceral branches of the abdominal aorta. The principle is their one-stage reconstruction. The types of reconstruction of these branches should be variable depending on the volume and extent of the pathological process.
9. Patients with aneurysmal lesion of abdominal aorta initially always have significant disorders of haemostasis system. In 30% of patients with occlusive diseases of aorta and its branches in the preoperative period the activity of thrombocytic-vascular link of hemostasis is increased, antithrombotic ability of vascular wall endothelium is decreased and blood rheological properties are disturbed. Activation of fibrinolysis was noted in patients with aneurysmal lesion of abdominal aorta.
10. During the operation for abdominal aortic aneurysmal lesion, after starting the blood flow the level of plasminogen increases additionally by 30%, which is a risk factor for haemorrhagic complications in the perioperative period. On the 1-3 day after the operation there is a significant decrease of blood anticoagulant potential - antithrombin-Sh by 25-27%, protein C by 23-25%. This period is the most dangerous in terms of thrombohemorrhagic complications development.
11. When using standard heparin during the operation there is a consumption of antithrombin-Sh by 30-45% and increase of platelet aggregation by 10%, which is a threatening condition for the occurrence of thrombosis of deep veins of the lower extremities with subsequent TELA. When using fraxiparin during reconstructive vascular surgeries the consumption of antithrombin-Sh and increase in platelet aggregation do not occur, prothrombin time, activated partial thromboplastin time, thrombin time are lengthened insignificantly that testifies to expediency of its use for prevention of thrombohemorrhagic complications.
12. Application of the diagnostic methods proposed by us to detect the main risk factors during the operation and in the nearest postoperative period, use of the algorithm of stage and volume of intervention allowed to reduce significantly the number of threatening complications, thus the lethality decreased 4 times, and the number of non-fatal complications - 4 times non-fatal complications - 1.5 times.