

Доктор ахборотномаси № 1—2020
86
DOI: 10.38095/2181-466X-2020931-86-88 УДК: 618.19-005.1-618.56-005.1
THE ROLE OF HEMOSTATIC SYSTEM INDICATORS
IN PREDICTING OBSTETRIC BLEEDING
N. R. Khamidova, M. N. Negmatullaeva, D. I. Tuksanova, F. K. Akhmedov
Bukhara state medical institute, Bukhara, Uzbekistan
Key words:
physiological pregnancy, D-dimer, fibrinolysis, hemostasiologic.
Таянч сўзлар:
физиологик ҳомиладорлик, Д-димер, фибринолиз, гемостазиологик.
Ключевые слова:
физиологическая беременность, D-димер, фибринолиз, гемостазиологический.
The purpose of the study: to evaluate the state of hem coagulation with its physiological course for predicting
the risk of obstetric hemorrhage in terms of trimesters of pregnancy in its dynamics. Surveyed 65 women with physio-
logical pregnancy. Of these, 30 women (group II) have risk factors; smoking patients during this pregnancy, over-
weight, taking oral contraceptives with the abolition of less than or 3 months before pregnancy. 35- Women without
risk factors with a normal pregnancy. Clinical and hemostasiologic studies were performed for periods of 10–12, 22–
24, and 35–36 weeks of gestation. During gestation, there was an increase in spontaneous platelets, an increase in fi-
brinogen level, D-dimer, and a slowdown in fibrinolysis.
АКУШЕРЛИК ҚОН КЕТИШИНИ БАШОРАТЛАШДА ГЕМОСТАЗ
КЎРСАТКИЧЛАРИНИНГ АҲАМИЯТИ
Н. Р. Хамидова, М. Н. Негматуллаева, Д. И. Туксанова, Ф. К. Ахмедов
Бухоро давлат тиббиѐт институти, Бухоро, Ўзбекистон
Тадқиқот мақсади: ҳомиладорлиги физиологик кечаѐтган аѐлларда динамикада акушерлик қон кетиши
хавфини башорат қилиш, учун қон ивишининг ҳолатини баҳолашдан иборат. Ҳомиладорлиги физиологик
кечаѐтган 65 нафар аѐл ўртасида текширув ўтказилди. Улардан 30 нафар аѐл (II гуруҳ) хавф омилларига эга;
ҳомиладорлик пайтида чекадиган, ортиқча вазнга эга бўлган, ҳомиладорликдан 3 ой олдин ѐки ундан 3 ой ол-
дин контрацептив воситаларни қабул қилган аѐллар. 35 - нафар эса хавф омиллари бўлмаган ҳомиладор аѐллар
олинди. Клиник ва гемостазиологик тадқиқотлар ҳомиладорликнинг 10–12, 22–24 ва 35–36 ҳафталарида ўтка-
зилди. Ҳомиладорлик пайтида ўз-ўзидан пайдо бўлган тромбоцитларнинг кўпайиши, фибриноген даражаси-
нинг ошиши, Д-димер ва фибринолизнинг секинлашиши кузатилди.
РОЛЬ ПОКАЗАТЕЛЕЙ СИСТЕМЫ ГЕМОСТАЗА В ПРОГНОЗИРОВАНИИ
АКУШЕРСКИХ КРОВОТЕЧЕНИЙ
Н. Р. Хамидова, М. Н. Негматуллаева, Д. И. Туксанова, Ф. К. Ахмедов
Бухарский государственный медицинский институт, Бухара, Узбекистан
Цель исследования: оценить состояние гемокоагуляции с ее физиологическим течением для
прогнозирования риска возникновения акушерских кровотечений в условиях триместра беременности в его
динамике. Обследовано 65 женщин с физиологической беременностью. Из них 30 женщин (группа II) имеют
факторы риска; Курящие пациенты во время этой беременности имеют избыточный вес, принимают оральные
контрацептивы с отменой менее чем за 3 месяца до беременности. 35- Женщины без факторов риска с нор-
мальной беременностью. Клинические и гемостазиологические исследования проводились в течение 10–12, 22
–24 и 35–36 недель беременности. Во время беременности наблюдалось увеличение спонтанных тромбоцитов,
повышение уровня фибриногена, D-димера и замедление фибринолиза.
Obstetric hemorrhages are the leading cause of maternal mortality in most countries of the
world, including our Republic of Uzbekistan. The frequency of obstetric bleeding with blood loss
of more than 1000 ml is from 2 to 8% in relation to the total number of births. Massive bleeding
due to a combination of several causes and almost always accompanied by gross violations of the
hem coagulation system [1,3,6].
Bleeding as the cause of maternal and prenatal mortality during pregnancy, in childbirth and
the postpartum period continues to be one of the urgent problems of modern obstetrics, being in 20
-28% of cases the only cause of deaths for the mother and fetus [4,5].
Massive bleeding may be due to a number of reasons and more often their combination. A
practical doctor is not always in the state of the variety of them to distinguish leading and imple-
ment the most rational prevention and therapy. The difficulty of real and differentiated prevention
of massive blood loss is due to several factors, one of the main factors being the presence of physi-
Оригинальная статья

Доктор ахборотномаси № 1—2020
87
ological hyper coagulation, as the ―pregnancy rate‖ [2,9,10].
However, the prognostic criteria for hemostatic system impairment resulting in massive ob-
stetric bleeding remain deeply unexplored. Changes in the hemostatic system of a pregnant woman
are physiological and are associated with the appearance of the uteroplacental circulation. This
process is due to various factors and is an adaptive response of the pregnant woman's div to com-
pensation of costs due to the development of the fetus and possible blood loss during childbirth.
An important indicator to characterize the degree of hemostasis activation is the level of D-
dimer. With fibrin cleavage, the final products are formed D-dimers. In healthy people, the con-
centration of D-dimer does not exceed 500 mg / ml FEV (units equivalent of fibrinogen). An ex-
cess of D-dimer indicates activation of fibrinolysis and an increase in the formation of thrombin
[7,8,10].
During normal pregnancy, the level of D-dimer in the blood plasma gradually increases sev-
eral times, reaching its peak by the first day of the postpartum period.
Excessive increase in D-dimer is considered evidence of the unfavorable course of pregnan-
cy and labor associated with impairment in the hemostasis system, including the development of
the risk of massive obstetric hemorrhage [8,9].
The study’s purpose:
to evaluate the state of hemocoagulation with its physiological course
for predicting the risk of obstetric hemorrhage in terms of trimesters of pregnancy in its dynamics.
Material and methods.
The study involved 65 women with physiological pregnancy. Of
these, 30 women (group II) have risk factors; smoking patients during this pregnancy, overweight,
taking oral contraceptives with the abolition of less than or 3 months before pregnancy. 35- Wom-
en without risk factors with a normal pregnancy. Clinical and hemostasiologic studies were per-
formed for periods of 10–12, 22–24, and 35–36 weeks of gestation. Clinical examination included
analysis of complaints, history taking, physical examination, analysis of medical records. Blood
for hemostasiological research was taken in the morning, on an empty stomach, from the cubital
vein, using a needle with a wide lumen. The study was carried out for 2 hours from the moment
the plasma was obtained on the ―Biologist 2A-230-2‖ apparatus. Coagulation studies were per-
formed using the ―Technology – Standard‖ reagents on a Diamed-CD-4 semi-automatic coagulom-
eter. Investigated activated plasma recalcification time (APR), activated partial prothromboplastin
time (APTT), prothrombin time (PT), fibrinogen level. Statistical processing of the results was car-
ried out using Student‘s criterion using the Statgraf and Microsoft Excel versions of the Windows
software package.
Results and discussion.
According to the inclusion criterion, 65 women were examined.
The average age of the patient is 25 (22-30) years. Of these, 30 had the first birth, 35 - repeated.
None of the patients before the survey did not receive anti-thrombotic therapy. The dynamics of
hemostasis are presented in the table below.
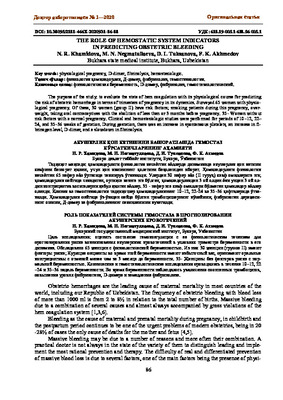
When analyzing the results obtained in the table it should be noted that, APR, АPTT, PT did
not have dynamic static differences in trimesters. At the same time, an increase in PV by the end
of pregnancy turned out to be statically significant compared with rates in the first and second tri-
mesters. Since this test reflects the total antithrombin plasma activity, it is possible that the in-
crease is due to an increase in the level of paracoagulation products, which have an anticoagulant
effect.
When analyzing the number of platelets, we found no statistical differences with a slight de-
crease in mean values in the third trimester, which can be explained by both relative hemodilution
and partial physiological consumption of platelets in the uteroplacental circulation.
It is noteworthy that there is an increase in the level of fibrinogen during pregnancy, which is
39.4% out of the normal range by the end of pregnancy compared with the first trimester. In paral-
lel with hyperfibrinogenemia, there was a threefold increase in the content of D-dimer, respective-
ly.
A comparative analysis of these parameters in the studied patients of groups I and II revealed
a 3.7% increase in the number of platelets, ABP decreased by 3.8%, APTT decreased by 3.6%, PT
N. R. Khamidova, M. N. Negmatullaeva,...

Доктор ахборотномаси № 1—2020
88
Note: Significance of differences (P <0.05) when comparing indicators: * in I and II trimesters, ** - in I and III
trimesters *** - in II and III trimesters.
Table 1.
Comparative indicators of hemostasis physiological course of pregnancy
and in pregnant women at risk.
increased by 5.6%. Indicators of D-dimers increased by 15.1% in the 3rd trimester in pregnant
women with an existing risk group (Group II).
Thus, indicators of fibrinogen, D-dimer and PV can be early markers of changes in the he-
mostasis system in patients with risk factors even during physiological pregnancy, and they can be
included in the group of pregnant women with a high risk of bleeding during childbirth. In order to
prevent the expected risks that exist, it is necessary to address the issues of prenatal hospitaliza-
tion, which require medical correction of hemostasis system parameters, in order to achieve a suc-
cessful outcome of labor for the mother.
References:
1. Bertina R.M. Molecular risk factor for thrombosis // Thrombosis and Haemostasis J. 2013. № 2 (82). P.601-
610.
2. Brenner B. Hemostatic changes in pregnancy // Thrombosis Research. P. 2014. Vol. 114. P. 409-414.
3. Halligan A., Bonnar J., Sheppard В., et al. Haemostatic, fibrinolytic and endothelial variables in normal preg-
nancy // Br. J. Obstet. Gynecol. 2014. № 6 (101). P. 488-492.
4. Kulikov, A.V. Emergency protocol for bleeding in obstetrics / A.V. Kulikov, S.V. Martirosyan, T.A. Obo-
Skalova. - Ekaterinburg, 2010. - 28 p.
5. Modern technologies for the treatment of obstetric hemorrhages / V. E. Radzinsky [and others] // Farmateka -
2010. - № 1. - P. 12-16.
6. Olson JD. D-dimer: An Overview of Hemostasis and Fibrinolysis, Assays, and Clinical Applications. Advances
in Clinical Chemistry. 2015;69:2-46. doi:10.1016/bs.acc.2014.12.001.
7. Opportunities for the prevention of massive blood loss in the postpartum period / V. A. Novikova [and oth-
ers] // Proceedings of the XIII All-Russian Scientific Forum "Mother and Child" September 25-28, 2012; edited
by G. T. Sukhikh. - M., 2012. - P. 124-125.
8. O‘Riordan M.N., Higgins J.R. Haemostasis in normal and abnormal pregnancy // Best Pract Res Clin Obstet
Gynaecol. 2013. № 3 (17). Р. 385-396.
9. Palareti G, Cosmi B, Legnani C, Antonucci E, De Micheli V, Ghirarduzzi A, Poli D, Testa S, Tosetto A, Pengo
V and Paolo Prandoni. D-dimer to guide the duration of anticoagulation in patients with venous thromboembo-
lism: a management study. Blood. 2014;124(2):196-203. doi:10.1182/blood-2014-01-548065.
10.Prevention of massive bleeding in obstetric practice / V.L. Silyava [and others] // Med. journals - 2012. - № 1. -
p. 77-81.
11.Schouten HJ, Geersing GJ, Koek HL, A Zuithoff N, Janssen K, Douma RA, van Delden JM, Moons K, Reits-
ma JB. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with sus-
pected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346:f2492. doi:10.1136/
bmj.f2492.
Оригинальная статья
Indicator
Trimester
I
II
III
I group
(n=30)
II group
(n=35)
I group
(n=30)
II group
(n=35)
I group
(n=30)
II group
(n=35)
Platelet count, 10
9
/L
235±36
230±34
225±39
220±30
218±30
213±25
Spontaneous plate-
let aggregation, %
0.17±0.13 0.16±0.15** 0.35±0.15** 0.40±0,17** 0.34±0.14** 0.30±0.12**
APR
(activated
plasma recalcifica-
tion time), s
56.1±5.1
55.1±4.9
57.6±5.4
58.5±5.1
56.9±5.3
54.8±5.4
АPTT (activated
partial thromboplas-
tin time), s
33.8±2.6
33.6±2.8
33.3±3.0
33.1±2.9
33.3±2.8
32.1±2.9
Fibrinogen, g/l
3.8±0.6
4.1±0.5
4.2±0.5*
4.8±0.4**
5.3±1.5**
5.8±1.6
Prothrombin time, s
15.5±0.9
15.9±0.8
15.7±1.2
16.1±1.1
16.1±1.8***
17±1.6***
D-dimer, mg/ml
115±58.6
125±60.2
276.8±5.1*
301±1,2
469±77.7
540±80.5***





